Click here for a downloadable PDF with citations
Testimony of David E. Mitchell Founder, Patients For Affordable Drugs NOW before the U.S. Senate Committee on the Judiciary for a hearing on “Ensuring Affordable & Accessible Medications: Examining Competition in the Prescription Drug Market”
May 21, 2024
Chairman Durbin, Ranking Member Graham, members of the committee. Thank you for inviting me to testify today at this important hearing examining how we can lower prescription drug prices by curbing the rampant anticompetitive conduct in prescription drug markets that is hurting patients, consumers, and taxpayers across America.
Section I. Background and Introduction
My name is David Mitchell. I am the founder of Patients For Affordable Drugs NOW. We are the only national patient advocacy organization focused exclusively on policies to lower prescription drug prices. We are independent, bipartisan and we don’t accept funding from any organizations that profit from the development or distribution of prescription drugs.
Since we launched a little over seven years ago, more than 35,000 patients across all 50 states have shared stories with us of their struggles to pay high drug prices. And we have built a community of more than three-quarters of a million patients and allies supporting policies to lower drug prices.
More importantly for today, I have an incurable blood cancer, and prescription drugs are keeping me alive — literally.
My oncologists currently have me on a four-drug combination of infused and oral cancer medications. These four drugs carry a combined list price of more than $1 million per year. Just one of my oral drugs, called Pomalyst, is priced at more than $22,400 for 21 capsules, which I must buy every 28 days. And because Medicare beneficiaries like me pay our out-of-pocket costs based on list price, I spent more than $16,500 out-of-pocket last year — just for Pomalyst. To help manage the cost of my infused drugs, I spend another $3,980 per year to purchase a Part B supplement. And of course, I have the base costs of Medicare to pay as well.
But the Inflation Reduction Act has changed that equation completely. After paying more than $16,000 last year because there was no out-of-pocket maximum in Part D, I am paying only $3,326 this year as an out-of-pocket cap began to phase in. Next year, the maximum anyone on Medicare will pay annually for drugs is $2,000. Our patients who have been unfortunate enough to contract a disease or condition requiring expensive drugs are elated–they say it is life-changing. Judy from Maine wrote to us a few weeks ago saying:
“I have to admit that I was still a bit skeptical about the Medicare changes until today. In January my copay for Enbrel was $2,150.83. In February it was $1,141.86. Today it was zero. I was thrilled, as was the staff at the pharmacy.”
That’s just one story. There are many more like that.
Here on this slide is the state of my disease today. This slide below is from a presentation to the FDA’s Oncologic Drugs Advisory Committee on March 15 of this year on the state of multiple myeloma in the U.S. Please note the last point.
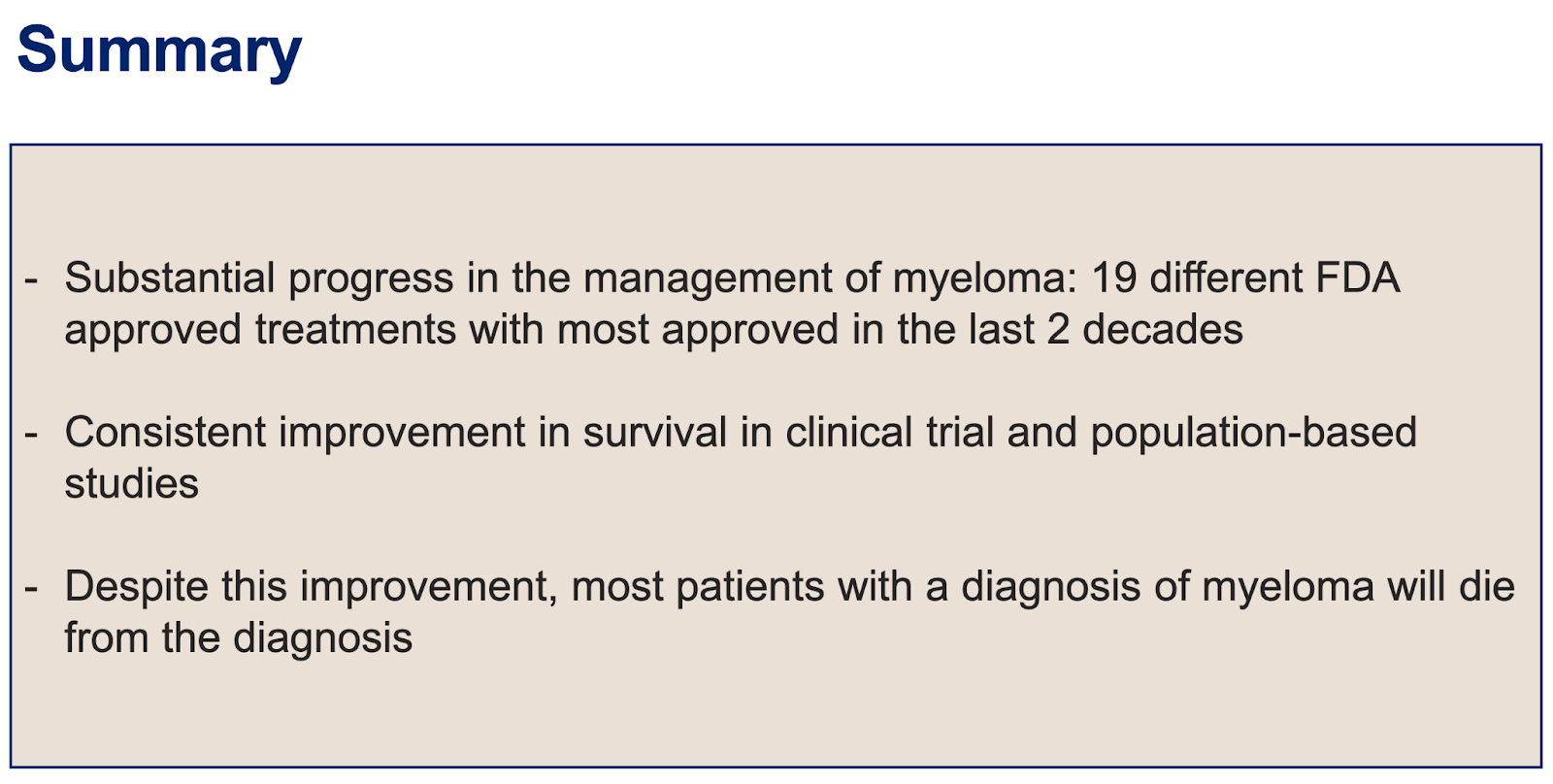
The last point is always sobering to reflect on: “Despite this improvement, most patients with a diagnosis of myeloma will die from the diagnosis.” Yet, I am a very lucky man — the drugs are currently keeping my cancer at bay, and I tolerate them pretty well. But with multiple myeloma, nothing works forever. This is why innovation is so important to me. And it goes to the heart of the reason for this hearing:
We rely on patents to incentivize and reward innovation. We give drug companies limited-time monopolies to charge whatever they like in order to ensure a rich reward for the development of innovative new drugs. We need that innovation. I need it personally. But drugs don’t work if people can’t afford them. And too often drug companies abuse the current patent system, not to reward innovation, but to block competition that would lower prices as the patent laws intend. The bipartisan bills that are the focus of today’s hearing aim to address that abuse and restore the intended balance.
For me personally, the point is: I need innovative new drugs. I care deeply about innovation and new drug development. My life depends on it. Without innovation, I will die sooner than I hope to. That is not a plea for sympathy–it’s just an unfortunate fact.
But my more than 13-year journey as a cancer patient has taught me that our current system which relies on competition and market forces to lower drug prices after a period of monopoly pricing is not working. I’m here to ask each of you to fix it.
Section II. The High Prices Americans Pay For Drugs and Need For Further Reforms
Drugs are too expensive in the United States. Americans pay more than four times what people in other wealthy nations pay for the exact same brand-name drugs. Even after applying estimated rebates to arrive at net prices, Americans are still paying more than three times what people in other wealthy nations pay for the same brand-name drugs.
Consequently, about three in ten Americans report having difficulty affording their medications. When their prescription drug prices are too high, Americans face challenges affording other expenses, such as food and housing. One survey found that over 20 percent of people took on debt or declared bankruptcy because of their medications.
High drug prices disproportionately harm communities of color. One in two Latinos in the United States takes a prescription medication, and more than 20 percent are uninsured. Black and Latino adults aged 65 and older were more likely to report difficulty affording prescription medications than White adults. Further, Black Americans are more likely to live with chronic pain, diabetes, and high blood pressure than white Americans and are nearly two times more likely to be uninsured.
As expensive as my drugs are, even with Medicare out-of-pocket caps taking effect, I never lose sight of the fact that roughly 26 million Americans don’t have any health insurance at all and are exposed to the full list price of the medications they need.
The reality is that people struggle to pay these high prices with and without insurance.
Americans have been demanding relief for years. A KFF poll in July of 2023 found three out of four Americans said there is not enough government intervention when it comes to limiting the price of prescription drugs. That includes 82 percent of Democrats, 67 percent of Independents, and 68 percent of Republicans. In the wake of the enactment of the Inflation Reduction Act which is helping millions of people by lowering prices and making drugs more affordable–Americans want more done.
Section III. The Need for Patent Reform
When a drug company makes a truly innovative discovery, it should be rewarded with a patent and receive a fair return for the risk and investment it undertook. Our patent system was created to facilitate these rewards for innovation so that drug companies are incentivized to pursue true clinical breakthroughs and inventions that bring meaningful benefits to patients.
But the drug industry would have you believe that every patent is deserved and that the sheer volume of patents granted is an appropriate indicator of innovative achievements. That couldn’t be further from the truth.
Neither new patents nor new drugs equal new innovation. Worse, in too many cases, manufacturers are abusing America’s patent and exclusivity system –not to reward innovation – but to prevent free-market competition and block affordable generic and biosimilar drugs from coming to market.
Between 2005 and 2015, 74 percent of the new drug patents issued were for drugs already on the market. A second study of the ten top-selling drugs in 2021 corroborated that number. Of the roughly 100 best-selling drugs in another study, nearly 80 percent obtained an additional patent to extend their monopoly period.
In fact, gaming of the patent system to extend monopolies beyond the time intended under law inhibits true innovation patients like me need. If big drug companies can block competition and raise prices on old drugs at will in order to drive profits and executive bonuses, they have far less incentive to take risks by investing in research and development (R&D) to develop innovative new drugs that could command high prices and save lives.
There are a variety of strategies used by drug corporations to extend monopolies, including product hopping, evergreening, patent thicketing, pay-for-delay deals, and abuse of the U.S. Food and Drug Administration (FDA)’s citizen petition process.
These tactics lead to longer exclusivity than our laws intend. The median length of post-approval market exclusivity for small-molecule drugs in one study was not five years or even the seven years allowed for orphan drugs. Instead, it was 12.4 years.
Product Hopping
Let’s start with product hopping. This tactic occurs when a brand-name company switches a patient population from an older product whose patent is coming to an end and facing imminent competition to a different formulation that has a later expiring patent and therefore, is not facing competition. The “new” drug typically offers little or no new clinical benefit, it may even be as simple as changing a product from a tablet to a capsule.
This switching takes two forms. In “hard” switches, the brand-name company removes the older product from the market, forcing patients onto the new version. With “soft” switches, the company keeps the older product on the market, but engages in aggressive marketing to prescribers and patients, urging them to switch to the newer formulation. By switching their market to a “new drug,” brand-name companies effectively eliminate the market for new generics that rely on automatic substitution state laws to gain traction in the patient populations.
As patients, we support product evolution that improves effectiveness or reduces toxicities of a drug. I take a drug that causes painful peripheral neuropathy—loss of feeling in my feet. If a reformulated drug were to reduce this type of side effect, it might well meet an appropriate standard for an innovative change meriting a patent extension.
Unfortunately, this is often not the case for patients. Two drugs that have been involved in high-profile product hopping cases are Suboxone and Tricor, which treat opioid dependence and high cholesterol respectively. Here’s what patients have told us about both:
Samantha from West Virginia writes:
“I have been in recovery for over ten years now. The cost of Suboxone is outrageous — especially since, from the time I began taking it until now, the price is still as high or higher. It’s ridiculous! It’s easier for people to misuse narcotics (the cost is less). The cost for Suboxone is about $800 [for a 90-day supply].”
Beatel from Minnesota told us:
“When I changed to Medicare at 65, my price for 40mg of Tricor went to $1,800/month. The pharmacist whispered to me, ‘If the doctor changed the order to 160 mg tabs and I broke it in half for the 80 mg dose, it would cost me $40.’ The drug company still had the patent on the 40mg tab. The patent for the 160mg tab had expired…same drug.”
Patent Thickets
Patent thicketing is a tactic similarly designed to undermine market competition at the expense of patients. This strategy occurs when drug companies file dozens of non-innovative patents in order to create an impenetrable “thicket” around a drug product forcing a prospective generic or biosimilar competitor to litigate through each of the patents in order to gain market entry.
Let’s look at another drug I take to prevent blood clots and stroke–Eliquis. In 2021, it was the most expensive drug for Medicare at $12.6 billion. Its maker-Bristol Myers Squibb (BMS) has applied for 48 patents and been granted 27, blocking competition in this country for 40 years. The list price for a 30-day supply in the U.S. is about $600. The cost in Canada–where there is a generic on the market–is less than $75.
The encouraging news is that there are multiple bills before the Senate designed to close loopholes in our patent system that are harming patients. All have bipartisan support. Many have already cleared this committee on strong bipartisan votes.
● P4ADNOW supports S. 150, the “Affordable Prescriptions for Patients Act of 2023,” which cracks down on patent thickets in the biologic market and is projected to save hundreds of millions of dollars. There is also a new bipartisan bill-S. 3583-which has not cleared committee and we support that bill as well.
● S. 150 also addresses product hopping. When combined with the legislation’s patent thicket provisions, the bill could save $1 billion.
● Pay-for-delay continues to be a problem, despite the Actavis decision. This tactic occurs when brand-name drug companies provide something of value to a potential competitor to induce them to delay selling a generic version of a drug, therefore keeping it off the market in order for the brand-name drug to maintain a monopoly for longer. P4ADNOW has endorsed S. 142, a bipartisan bill to curb pay-for-delay agreements that the nonpartisan Congressional Budget Office (CBO) estimates could save $600 million.
● The citizen petition process at the FDA was designed so that patients could raise safety concerns about drug approvals. But research has revealed that the citizen petition process has been co-opted by corporations looking to block competition. Brand-name drug makers were behind 92 percent of all citizen petitions filed between 2011 and 2015. But they were not raising legitimate safety concerns, which is why the FDA threw out nine of every 10 of the industry’s “sham” petitions, which were without scientific merit and filed for the sole purpose of delaying generic competition, keeping prices high for patients. P4ADNOW supports both S. 148 and S. 1067 which will reform this process, promote generic competition, and save millions of dollars.
● Current FDA policies prohibit the agency from disclosing information generic companies need in order to speed approval of new generic competitors. P4ADNOW supports S. 775 which will increase transparency and facilitate generic entry. This bill is projected to save more than $800 million.
● P4ADNOW also supports S. 79 which will establish a task force between the United States Patent and Trademark Office (USPTO) and FDA in order to improve communication in the implementation of each agency’s patent-related activities.
To achieve true innovation at prices that are affordable over the long haul, we must reform our patent and exclusivity system so that it is once again focused on driving innovation that saves lives, not driving high prices that make lifesaving drugs unaffordable to those whose lives depend on them.
Section IV. What Else Should We Do? Reform Pharmacy Benefit Managers (PBMs)
While the headwaters of our drug pricing problems are the list prices set by drug corporations, there are other reforms needed downstream in the supply chain. Pharmacy benefit managers (PBMs) are black boxes that cut secret, mutually beneficial rebate deals with manufacturers, and none of it is transparent. We need to increase transparency and curb anticompetitive practices by PBMs.
It is simply wrong that patients like me don’t know if the preferred drug on a PBM formulary is there because it is the best drug, because it is the least expensive drug among equally effective options, or because the PBM got a big, legal kickback from the manufacturer. Without transparency, it is impossible to know how much of a rebate is going to the PBM, to the insurer, to lower my premiums, or to reduce my out-of-pocket costs at the pharmacy counter. With the Big Three PBMs–Cigna, Optum Rx, and CVS Health–in control of 80 percent of the $633 billion in U.S. spending on drugs, that is more than half a trillion dollars flowing through just those three entities annually., And vertical integration uniting all three major PBMs with insurers only increases their market power. Opaque practices with that kind of money involved are a bad way to run a railroad. It’s time for transparency to ensure PBMs are operating in the best interests of patients and consumers.
It’s not just about transparency either. Drug companies and PBMs also enter into rebate arrangements that are designed to thwart lower-cost competition. These are commonly called “rebate walls,” defined as:
“Exclusionary contracting practices that a drug manufacturer deploys to limit the ability of rivals from gaining preferred access to the formulary, or any access at all. Branded manufacturers leverage their position as market leaders by offering financial incentives to pharmacy benefit managers and health insurers in the form of ‘all or nothing’ conditional volume-based rebates, in exchange for virtually exclusive positioning on the formulary. …If the payer does not accept the rebate agreement for a particular indication, it may lose all rebates for its product on all covered indications.”
Let’s be clear: These rebate deals are designed to benefit both the manufacturer seeking to block competition and the PBM that gets a bigger rebate. These deals are not designed to help patients like me by lowering prices or increasing patient choice. They are emblematic of our drug pricing system which has been built to benefit those who profit from it at the expense of those it is supposed to serve.
P4ADNOW supports reforming the practices of PBMs, including transparency requirements in order to determine how rebates are actually working — how much is going to reduce premiums and out-of-pocket for patients and consumers and how much is going to increase profits for the PBMs or insurer plan managers. In our ideal world, PBMs would have a fiduciary responsibility to patients and all beneficiaries, and all reforms would put patients at the center. While none of the PBM bills go as far as we would like, each takes important steps in the right direction and would make meaningful and important progress in the regulation and oversight of PBMs. We support key provisions of bills that have cleared the Finance Committee on unanimous or near-unanimous bipartisan votes:
The House Energy and Commerce Committee has also advanced legislation addressing PBM practices. We support provisions in the Lower Cost, More Transparency Act, H.R. 5378, that improve transparency and reporting requirements. We were also pleased to see the House Ways and Means Committee include reform delinking PBM compensation from prices in legislation it advanced earlier this month – H.R. 8261, the “Preserving Telehealth, Hospital, and Ambulance Access Act. In our view, however, none of the provisions in House legislation go far enough in reforming PBMs and ensuring they are putting patients and consumers first.
We are also following closely and supporting the Federal Trade Commission (FTC) investigation into PBMs as well. We look forward to the first interim report on that investigation expected this summer. We hope Congress uses the report to inform future legislation, and that Congress gives strong backing for the FTC to take action it may recommend.
Section V. The Inflation Reduction Act Strikes A Balance To Ensure Innovation We Need At Prices We Can Better Afford
It’s important to note that the Inflation Reduction Act (IRA) is built to strike a balance to ensure the innovation we need at prices we can better afford. In the run-up to the enactment of the IRA, the drug industry kept telling us that the legislation would stifle investment and kill innovation and access to new drugs. No one cares more about innovation than patients. But if you pull back the curtain on this pharma fear-mongering and look at what has actually happened since the IRA enactment, the argument doesn’t hold up. Here are eight reasons why.
The industry has plenty of money for innovation. In the wake of the Inflation Reduction Act passage, investors are upbeat. Drug company stocks are doing fine. The industry is flush with cash and has great access to capital.
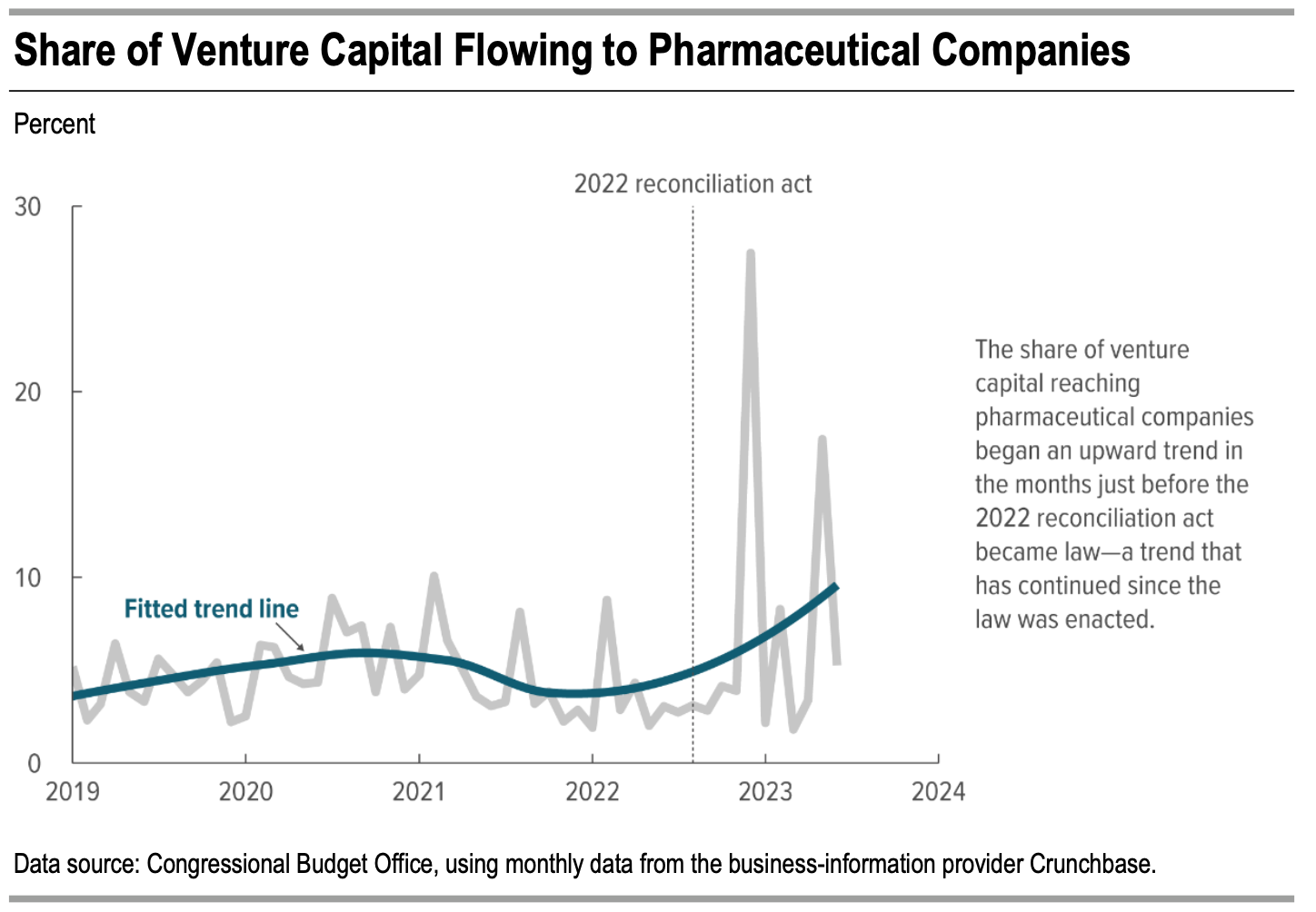
According to the Congressional Budget Office (CBO), despite Big Pharma’s claims that the implementation of the Inflation Reduction Act would stifle innovation and significantly impact profit margins, there has been a consistent and continuous increase in venture capital investment in pharmaceutical companies, demonstrating stability and resilience within this sector as shown in Figure 1.
Figure 1.
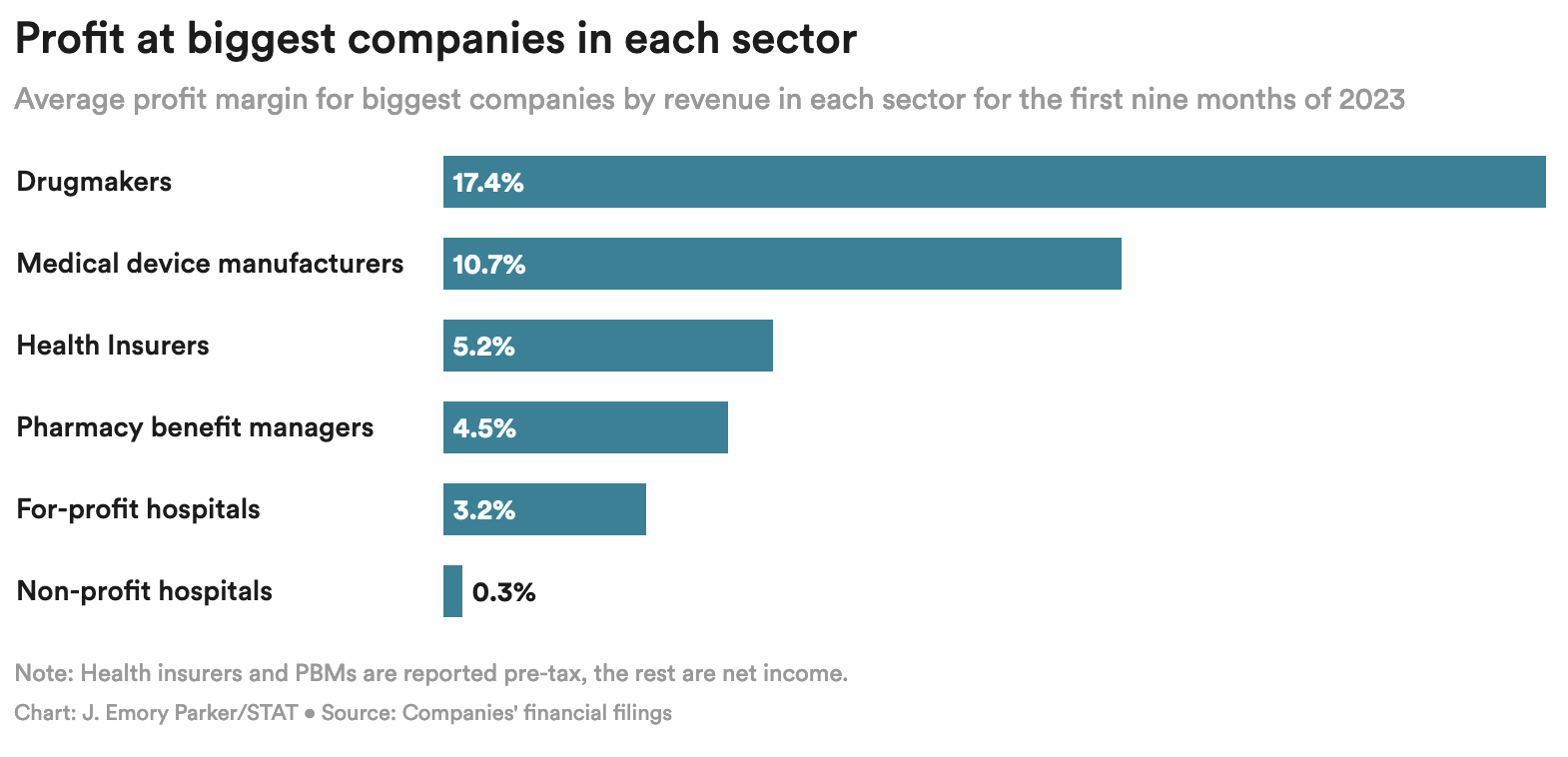
Drug companies remain by far and away the most profitable sector of the healthcare industry–more than tripling the profit of Pharmacy Benefit Managers (PBMs) and insurers.
Figure 2.
Since the passage of the Inflation Reduction Act:
The Inflation Reduction Act incentivizes innovation by curbing drug companies’ ability to drive profits by raising prices on old drugs at will.
The Congressional Budget Office (CBO) says the Inflation Reduction Act will have a minimal to non-existent impact on new drug development.
Figure 3.

Taxpayers are the source of early high-risk, basic science that drives innovation — not industry.
Lower drug prices help people access existing, innovative drugs they need right now, but can’t afford.
Finally, Big Pharma consistently threatens that patients will lose access to newly developed drugs. It notes that more drugs are available — and are available faster — in the United States than in other wealthy countries. Pharma frequently cites a white paper from the White House Council of Economic Advisers (CEA) to explain why: “Drug manufacturers usually pursue market access in the United States before other markets due to the higher prices in the United States.” The CEA could also have mentioned the other big reason drug companies file for approval first in the United States: It is the largest market in the world., After the IRA is fully implemented our country will still offer the highest prices by far in the largest market in the world, preserving the incentive to file first for approval in the United States.
There are other important policies in the U.S. drug pricing system that lead to more drugs being available here compared to other countries, none of which are altered by lowering prices under the IRA:
Medicaid must cover every drug offered by a manufacturer in the United States if the manufacturer agrees to give Medicaid a best-price guarantee.
The pharmaceutical industry’s threats to innovation and access don’t hold up. The IRA restores balance to move us in the direction of fair prices and profits while still getting the innovation we need.
Section VI: Conclusion
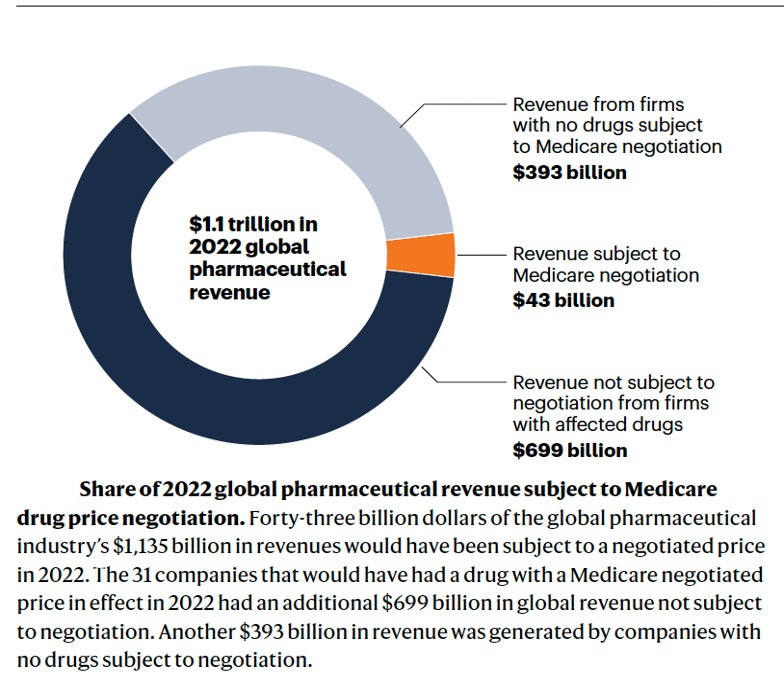
Let’s be clear: Big Pharma is not fighting for the interest of patients or because lowering its prices a bit will cripple innovation. It’s fighting to restore and maintain its complete economic power over the American people to dictate prices of brand-name drugs–a power it has in no other nation on the planet. The head of the powerful trade association, PhRMA, affirmed that fact in a moment of candor when he said in an interview a couple of years ago that his industry is “particularly adept at … rolling the tanks, if you will, to push back against policy proposals adverse to the industry’s interests.” The industry’s multiple lawsuits to block Medicare negotiation that will touch only about four percent of its global revenue is further evidence this struggle is about keeping the U.S. market as the one place in the world where it can dictate prices at the expense of people’s lives and livelihoods.
Of course, drug companies want to disguise that truth. Instead, they blame others and never offer policy solutions that involve lowering their prices. They seek to distract attention from their central role in making drugs unaffordable in America today.
And they try to scare us by saying that if we don’t bend to their will, we won’t get the drugs we need for the future. They pose questions like: How much would you pay to save a life?
And that’s easy. When it’s you or someone you love, the answer is anything. You’ll empty your bank account, mortgage your home, cash out your 401k. You’ll do whatever you have to do.
But that’s the wrong question. We should be asking: How do we strike and maintain a balance to ensure we get the innovation we need at prices we can afford?
While we at Patients For Affordable Drugs NOW would have gone further in the Inflation Reduction Act, it clearly was built with the goal of striking that balance as a foundational principle. That point is driven home by a fact that is worthy of repeating: The IRA does not change the key way our nation rewards investment and risk-taking for innovation–we continue to allow drug companies to set launch prices and maintain those prices for a minimum of nine to 13 years before potentially facing negotiated prices.
This story from John in Baltimore captures so well the challenges patients face and the need to lower drug prices. Like me, he has multiple myeloma and must take very expensive drugs. He says: “I’m on a tightrope that is scarier than the disease itself. I did everything to protect myself and my family from financial disaster, but I feel as though after everything I’ve been hijacked by a drug company. I have no other options and they want to keep it that way.”
I feel incredibly grateful to spend my retirement fighting so John can feel secure in his retirement, and not be held hostage by a drug company. I ask that you help John and millions of other Americans by moving forward with bipartisan patent and PBM reforms to make our system work better for the people it is supposed to serve.
Thank you.
Click here for a downloadable PDF
Statement of David E. Mitchell Founder, Patients For Affordable Drugs Now to the Subcommittee on Health of the United States House Of Representatives Energy and Commerce Committee for a hearing on “Legislative Proposals to Support Patients with Rare Diseases”
February 29, 2024
Section I. Background and Introduction
I want to thank you for holding this hearing “to discuss solutions to support patients living with rare diseases.” I am one of those patients. My name is David Mitchell. I am the founder of Patients For Affordable Drugs Now. We are the only national patient advocacy organization focused exclusively on policies to lower prescription drug prices. We are independent, bipartisan and we don’t accept funding from any organizations that profit from the development or distribution of prescription drugs.
Since we launched seven years ago, we have collected over 34,000 stories from patients across all 50 states struggling to pay high drug prices. And we have built a community of over three-quarters of a million patients and allies supporting policies to lower drug prices.
More importantly for today, I am a rare disease patient. I have a rare, incurable blood cancer, and prescription drugs are keeping me alive — literally.
My oncologists currently have me on a four-drug combination of infused and oral cancer drugs. These four drugs carry a combined list price of more than $1 million per year. Just one of my oral drugs, called Pomalyst, is priced at more than $22,400 for 21 capsules, which I must buy every 28 days. And because Medicare beneficiaries like me pay our out-of-pocket costs based on list price, I spent more than $16,500 out-of-pocket last year — just for Pomalyst. To help manage the cost of my infused drugs, I spend another $3,731 per year to purchase a Part B supplement. And of course, I have the base costs of Medicare to pay as well.
For people with my cancer — multiple myeloma — drugs account for 60 percent of the cost of treatment. Sixty percent.
I am a very lucky man — these drugs are currently keeping my cancer at bay, and I tolerate them pretty well. But the reason I am on four drugs is because each began to stop working, so the doctors first increased the dose, then increased the frequency, and then added another drug. Eventually, I will fail on this combination, too. When that happens, I will be what is called “triple refractory” to all of the three major classes of drugs used to treat my disease. The cancer will begin to increase in my blood and I will need a new treatment. Fortunately, there are options out there.
But one of the new drugs approved recently that I might be a candidate for carries a list price of $465,000. That’s just for the drug — it doesn’t cover the hundreds of thousands of dollars required to administer the drug and manage my health in the wake of the treatment. And each of the new drugs comes with its own risks: The treatment I am referring to is called Chimeric Antigen Receptor T-Cell therapy (CAR-T) and it carries a black box warning that it may actually cause secondary cancers. I don’t know what’s ahead in my journey as a cancer patient.
But the point is: I need these innovative new drugs. I care deeply about innovation and new drug development. My life depends on it. Without innovation, I will die sooner than I hope to. That is just an unfortunate fact.
But my more than 13-year journey as a cancer patient has taught me one irrefutable fact: Drugs don’t work if people can’t afford them.
Section II. The Price of Drugs and Need for Further Reforms
Drugs are too expensive in the United States, and there is no justification for the high prices. When drug makers hike prices each year, they don’t do so because the drug becomes more valuable. Drug companies raise prices because they can. We let them.
The result is that Americans pay more than four times what people in other wealthy nations pay for the exact same brand-name drugs. Even after applying an estimate of rebates to arrive at net prices, Americans are paying more than three times what people in other wealthy nations pay for the same brand name drugs.
Consequently, about three in ten Americans report having difficulty affording their medications. When their prescription drug prices are too high, Americans face challenges affording other expenses, such as food and housing. One survey found that over 20 percent of people took on debt or declared bankruptcy because of their medications.
High drug prices disproportionately harm communities of color. One in two Latinos in the United States takes a prescription medication, and more than 20 percent are uninsured. Black and Latino adults aged 65 and older were more likely to report difficulty affording prescription medications than White adults. Further, Black Americans are more likely to live with chronic pain, diabetes, and high blood pressure than white Americans and are nearly two times more likely to be uninsured.
As expensive as my drugs are, even with Medicare, I never lose sight of the fact that roughly 26 million Americans don’t have any health insurance at all and are exposed to the full list price.
People struggle to pay the prices with and without insurance.
Americans have been demanding relief for years. A KFF poll in July of 2023 found three out of four Americans said there is not enough government regulation when it comes to limiting the price of prescription drugs. That includes 82 percent of Democrats, 67 percent of Independents, and 68 percent of Republicans. In the wake of the enactment of the Inflation Reduction Act which is helping millions of people–Americans want more done.
Section III. The Inflation Reduction Act Is A Huge Step Forward Helping Millions Of People
The historic Inflation Reduction Act (IRA) is lowering prescription drug prices and reducing out-of-pocket costs for millions of people in this country. The benefits include:
“The Inflation Reduction Act’s redesign of Medicare Part D, including a $2,000 out-of-pocket cap is estimated to reduce enrollee out-of-pocket spending by about $7.4 billion annually among more than 18.7 million enrollees (36 percent of Part D enrollees) in 2025 – nearly $400 per person among enrollees who have savings in out-of-pocket costs under the IRA.” The IRA annual Medicare out-of-pocket spending limits began to phase in this year, and people taking expensive brand-name drugs will see their spending capped at the catastrophic level at about $3,300-3,500.
Let me tell you about my personal experience with the phasing in of the out-of-pocket cap this year. My total out-of-pocket expense for all my Medicare Part D drugs last year was $16,916 because there was no out-of-pocket cap in place. This year, thanks to the IRA’s phasing in of an out-of-pocket cap for beneficiaries who reach the catastrophic phase of the benefit this year, I paid $3,308 for my first fill of Pomalyst and will be paying no more out-of-pocket for Pomalyst or any of my Part D drugs for the rest of the year. That’s a savings of more than $13,600. For so many patients who are stuck with diseases or chronic conditions that require high-priced brand drugs, it is life-changing.
Take Sue from Wilmington, Delaware. She writes: “I have Waldenstroms Macrobulemia, a form of blood cancer. I take Imbruvica which is $18,000 a month. After insurance, I pay the first $8,000 in 2-months copay and then $1,000 a month thereafter. I am 76 years old and working full time to afford this medication.” Sue will save between $12,000-14,000 this year with the out-of-pocket cap phasing in.
It’s critical to remember that the way out-of-pocket costs are being reduced without unacceptable premiums or tax increases is by lowering the underlying prices of drugs in Medicare. If Congress weakens the IRA allowing higher prices than the law as written will deliver, we will see higher costs to both beneficiaries like Sue and myself, the government, and taxpayers.
Section IV. The Inflation Reduction Act Achieves Balance To Ensure Innovation We Need At Prices We Can Better Afford
In the run-up to the enactment of the IRA, the drug industry kept telling us that the legislation would stifle investment and kill innovation and access to new drugs. No one cares more about innovation than patients. But if you pull back the curtain on this pharma fear-mongering and look at what has actually happened since the IRA enactment, the argument doesn’t hold up. Here are nine reasons why.
The industry has plenty of money for innovation. In the wake of the Inflation Reduction Act passage, investors are upbeat. Drug company stocks are doing fine. The industry is flush with cash and has great access to capital.
According to the Congressional Budget Office (CBO), despite Big Pharma’s claims that the implementation of the Inflation Reduction Act would stifle innovation and significantly impact profit margins, there has been a consistent and continuous increase in venture capital investment in pharmaceutical companies, demonstrating stability and resilience within this sector as shown in Figure 1.
Figure 1.
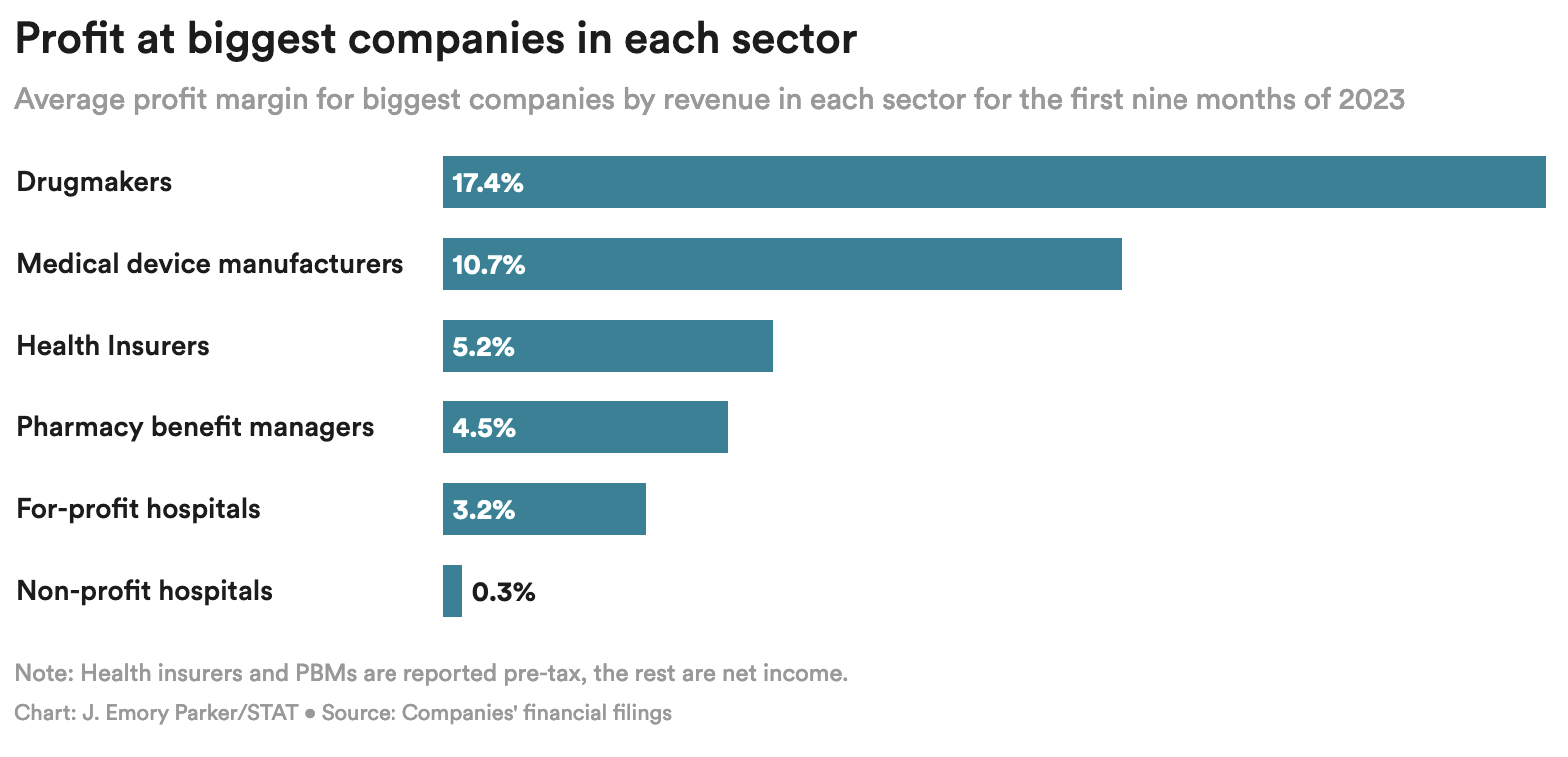
Drug companies are flush with cash and remain by far and away the most profitable sector of the healthcare industry–more than tripling the profit of Pharmacy Benefit Managers (PBMs) and insurers.
Figure 2.
Since the passage of the Inflation Reduction Act:
The Inflation Reduction Act incentivizes innovation by curbing drug companies’ ability to drive profits by raising prices on old drugs at will.
The Congressional Budget Office (CBO) says the Inflation Reduction Act will have a minimal to non-existent impact on new drug development.
Figure 3.
Taxpayers are the source of early high-risk, basic science that drives innovation — not industry.
Lower drug prices help people access existing, innovative drugs they need right now, but can’t afford.
The American public no longer buys Big Pharma’s threats to innovation. Policymakers shouldn’t fall for them either.
Finally, Big Pharma consistently threatens that patients will lose access to newly developed drugs. It notes that more drugs are available — and are available faster — in the United States than in other wealthy countries. Pharma frequently cites a white paper from the White House Council of Economic Advisers (CEA) to explain why: “Drug manufacturers usually pursue market access in the United States before other markets due to the higher prices in the United States.” The CEA could also have mentioned the other big reason drug companies file for approval first in the United States: It is the largest market in the world., After the IRA is fully implemented our country will still offer the highest prices by far in the largest market in the world, preserving the incentive to file first for approval in the United States,
There are other important policies in the U.S. drug pricing system that lead to more drugs being available here compared to other countries, none of which are altered by lowering prices under the IRA:
Medicaid must cover every drug offered by a manufacturer in the United States if the manufacturer agrees to give Medicaid a best-price guarantee.
The pharmaceutical industry’s threats to innovation and access don’t hold up. The IRA restores balance to move us in the direction of fair prices and profits while still getting the innovation we need.
Section V. H.R. 5547 and H.R. 5539 Are Misguided Because They Are Based On False Premises
H.R. 5547 is a solution in search of a problem that doesn’t exist in actuality and is only being raised by the industry to reduce the impact of Medicare negotiation and keep prices on more drugs higher for longer. The supposed problem posited by industry is that relative to the previous law, the reforms in the Inflation Reduction Act economically disadvantage small-molecule drugs compared to biologics, which will hurt innovation, increase prices, and harm the people who need these medicines.
This claim is completely misleading, and unsupported by the facts. The Inflation Reduction Act actually narrows the advantage for biologics over small molecules.
The pharma industry’s complaint is specious, which can be seen clearly in that, over time, its stances have been completely inconsistent. Biologics were given a huge advantage over small-molecule medicines because the pharmaceutical industry insisted on receiving seven years more market exclusivity for biologics than for small-molecule drugs when the Biologics Price Competition and Innovation Act (which was included in the Affordable Care Act) was being structured., , ,
Here’s what the trade association BIO said to justify a longer period of exclusivity for biologic drugs:
“Biologics research and development is a high-risk endeavor, with higher capital costs, higher material costs, greater manufacturing costs and uncertainties, longer development times, and lower late-stage success rates than compared to small molecule drugs.”
At the time, the pharmaceutical industry did not suggest that this enormous advantage for biologics would lead to the development of fewer small-molecule drugs, which it didn’t. Since 2010, more than 75 percent of new drugs approved by the FDA have been small molecules.
The Inflation Reduction Act actually contains more generous incentives for small-molecule medicines because it narrows the difference in years of exclusion from Medicare negotiation between biologics and small molecules to four years. And the negotiation exemption periods for small molecules (nine years) and biologics (13 years) are longer than the existing market exclusivity periods granted by the Food and Drug Administration (FDA), which are five years and 12 years, respectively.
Drug companies now assert that both types of drugs should be treated equally for purposes of negotiation — pharma’s chosen solution is, naturally, to increase the exemption period for small molecules to 13 years to match that of biologics. To put this into perspective, other high-income countries provide small-molecule and biologic drugs with identical periods of market exclusivity. The only reason the U.S. is not on that list is because the pharma industry lobbied the United States Congress aggressively for a longer monopoly period for biologics.
This misleading complaint — that the Inflation Reduction Act will stifle the development of small molecule drugs — is not supported by facts and is inconsistent relative to the pharmaceutical industry’s long-held positions on the need for advantageous treatment for biologic drugs.
In fact, since the enactment of the IRA, investment in small molecules has not declined–it has increased and investors are bullish:
The so-called “pill penalty” seems simple on its face, which no doubt is part of the reason pharma picked it as a rallying cry. But, if you do the math, it’s easy to see just how ridiculous the industry argument is. Drug companies will still continue to make massive profits on small molecules. To qualify for negotiation, a drug must, among other things, have annual Medicare sales of at least $200 million. Given that Medicare accounts for roughly 30 percent of total U.S. sales, an eligible drug would have more than $600 million in annual U.S. sales. Nine years of sales at $600 million annually produces revenue of more than $5.4 billion. Based on independent research, it costs an average of less than a billion dollars to bring a new drug to market–including covering costs of failures. That means a company with a drug qualifying for negotiation can easily make more than a 500 percent return on a small molecule before facing negotiated prices in Medicare. In fact, this simple math exercise greatly underestimates how much revenue these small molecule drugs can command when you consider that in 2023 average sales of small molecule drugs protected by exclusivity with over $200 million in annual revenue and nine or more years on the market is actually $2.86 billion.
The simple fact is that healthy profit is guaranteed on safe and effective small-molecule drugs because the IRA allows drug companies to set initial launch prices. That is the principal way we reward risk and investment to bring an innovative drug to market, and nothing in the IRA changed that core element of our system. Companies can set prices to ensure a healthy return before possibly being selected for negotiation. It is a no-lose proposition.
All of these points apply to the gene technologies that are the focus of H.R. 5547. With 5,000 gene therapy trials listed at the NIH–if only 10 percent come to market, mandating 13 years of exclusivity instead of nine years before negotiated prices take effect would raise Medicare spending dramatically.
The whole argument about 9 vs 13 years is not really about the interests of the millions of Americans who rely on medicines to get healthy — or stay alive. The drug industry simply wants 13 years of exemption from negotiated prices for all drugs to make as much profit as possible. Period. If drug companies now want equal timing for the negotiation of all drugs, we should equalize them all at nine years.
H. R. 5539 proposes to undo a critical reform in the IRA to ensure drug companies can’t abuse orphan drug status.
This issue deeply affects patients including myself. I have an orphan disease and three of the four cancer drugs I am currently taking were initially approved as orphan drugs–Velcade, Darzalex, and Pomalyst., , We need to protect incentives for orphan drug development, but we must stop the abuse of the orphan drug designation which extends monopolies indefinitely and hurts patients through the imposition of unjustified high prices.
The abuse of orphan status by drug companies was documented in detail by Kaiser Health News (KHN now KFF News) more than seven years ago. Here is a key conclusion from that investigation:
“‘What we are seeing is a system that was created with good intent being hijacked,’ said Bernard Munos, a former corporate strategy advisor at drug giant Eli Lilly and Co. who reviewed the KHN analysis of several FDA drug databases. It’s ‘quite remarkable that it has gone on for so long.’”
It’s time for the abuse to stop while protecting key incentives for orphan drug development, and that is exactly what the Inflation Reduction Act does.
Consistent with the overall approach of the IRA, the orphan drug provisions strike a balance that will stop abuse of patients by drug companies while still maintaining strong incentives for continued orphan drug development.
Section VI. What Else Should We Do? Curb Patent Abuse and Reform Pharmacy Benefit Managers (PBMs)
Patents For Innovation–Not To Block Competition and Lower Prices
When a drug company makes a truly innovative discovery, it should be rewarded with a patent and receive a fair return for risk and investment. Our patent system is designed to facilitate these rewards for innovation so that drug companies are incentivized to pursue true clinical breakthroughs and inventions that bring meaningful benefits to patients.
But the drug industry would have you believe that every patent is deserved and that the sheer volume of patents granted is an appropriate indicator of innovative achievements. That couldn’t be further from the truth.
Neither new patents nor new drugs equal new innovation. Worse, manufacturers are abusing America’s patent and exclusivity system in too many cases to prevent free-market competition and block affordable generic and biosimilar drugs from coming to market.
Between 2005 and 2015, at least 78 percent of the new drug patents issued were for drugs already on the market.
Of the roughly 100 best-selling drugs, nearly 80 percent obtained additional patents to extend their monopoly period.
In fact, gaming of the patent system to extend monopolies beyond the time intended under law inhibits true innovation that patients like me and millions of others need. If drug companies can block competition and raise prices at will on old drugs to drive profits and executive bonuses, they have far less incentive to take risks and invest in Research and Development (R&D) to find innovative new drugs that could command high prices and save lives.
There are a variety of strategies used by drug corporations to extend monopolies, including product hopping, patent thicketing, pay-for-delay deals, and abuse of the Food and Drug Administration’s (FDA) citizen petition process. All of these practices thwart competition and allow drug corporations to keep drug prices high. There have been several bipartisan pieces of legislation advanced in this Congress to address these issues and allow for more generic drugs and biosimilars to enter the market, which is critical to making drugs more affordable for patients.
P4ADNow strongly supports H.R. 3839, which was included in the Lower Costs, More Transparency Act, and passed the House on a strong bipartisan vote. In addition, P4ADNow supports bipartisan legislation that would reduce patent thicketing, curb product hopping, ban pay-for-delay agreements, reduce abuse of citizen petitions at the FDA, and improve coordination between FDA and the US Patent Trademark and Office (USPTO). Importantly, all of these measures would produce billions of dollars in savings that could be used to offset other health care priorities.
We must ensure patents are used as intended to reward true invention and innovation–not to extend monopolies and block lower prices through competition. To achieve true innovation at prices we can afford over the long haul, we must reform our patent and exclusivity system.
Increase Transparency and Stop Anticompetitive Practices By Pharmacy Benefit Managers (PBMs)
While the headwaters of our drug pricing problems are the list prices set by drug corporations, there are other reforms needed downstream in the supply chain. Pharmacy benefit managers (PBMs) are black boxes that cut secret, mutually beneficial rebate deals with manufacturers, and none of it is transparent.
It is simply wrong that patients like me don’t know if the preferred drug on a PBM formulary is there because it is the best drug, because it is the least expensive drug among equally effective options, or because the PBM got a big, legal kickback from the manufacturer. Without transparency, it is impossible to know how much of a rebate is going to the PBM, to the insurer, to lower my premiums, or to reduce my out-of-pocket costs at the pharmacy counter. With the Big Three PBMs–Cigna, Optum Rx, and CVS Health–in control of 80 percent of the $633 billion in U.S. spending on drugs, that is more than half a trillion dollars flowing through just those three entities annually., And vertical integration uniting all three major PBMs with insurers only increases their market power. Opaque practices with that kind of money involved are a bad way to run a railroad. It’s time for transparency to ensure PBMs are operating in the best interests of those they are supposed to serve — patients and consumers.
Drug companies and PBMs also enter into rebate arrangements that are designed to thwart lower-cost competition. These are commonly called “rebate walls,” defined as:
“Exclusionary contracting practices that a drug manufacturer deploys to limit the ability of rivals from gaining preferred access to the formulary, or any access at all. Branded manufacturers leverage their position as market leaders by offering financial incentives to pharmacy benefit managers and health insurers in the form of ‘all or nothing’ conditional volume-based rebates, in exchange for virtually exclusive positioning on the formulary. …If the payer does not accept the rebate agreement for a particular indication, it may lose all rebates for its product on all covered indications.”
Let’s be clear: These deals are designed to benefit both the manufacturer seeking to block competition and the PBM that gets a bigger rebate. These deals are not designed to help patients like me by lowering prices or increasing patient choice. They are emblematic of our drug pricing system which has been built to benefit those who profit from it at the expense of those it is supposed to serve.
P4ADNow supports reforming the practices of PBMs, including transparency requirements in order to determine how rebates are actually working — how much is going to reduce premiums and out-of-pocket for patients and consumers and how much is going to increase profits for the PBMs or insurer plan manager.
We’re pleased that the Lower Costs, More Transparency Act included several provisions to improve PBM transparency and eliminate spread pricing, among other elements. We also support reforms to “de-link” administrative fees from drug prices and to pass more of the savings collected through negotiated discounts along to patients and consumers whether through lower prices, lower out-of-pocket, or lower premiums. We hope that Congress will consider many of these measures for inclusion in upcoming health care legislation.
We are also following closely and supporting the Federal Trade Commission (FTC) investigation of these issues as well. We hope Congress will ensure the ability of the FTC to seek damages and monetary penalties for consumer protection and competition cases.
Section VII: Conclusion
Let’s be clear: Big Pharma is not fighting for the interest of patients or because lowering its prices a bit will cripple innovation. It’s fighting to maintain its economic power over the American people to dictate prices of brand-name drugs–a power it has in no other nation on the planet. The head of the powerful trade association, PhRMA, affirmed that fact in a moment of candor when he said in an interview not long ago that his industry is “particularly adept at … rolling the tanks, if you will, to push back against policy proposals adverse to the industry’s interests.” The industry’s multiple lawsuits to block Medicare negotiation that will touch only about four percent of its global revenue is further evidence this struggle is about keeping the U.S. market as the one place in the world where it can dictate prices at the expense of people’s lives and livelihoods.
Of course, Big Pharma wants to disguise that truth. Instead, it blames others and distracts attention from its central role in making drugs unaffordable.
And it tries to scare us by saying that if we don’t bend to its will, we won’t get the drugs we need for the future. It poses questions like: How much would you pay to save a life?
And that’s easy. When it’s you or someone you love, the answer is anything. You’ll empty your bank account, mortgage your home, cash out your 401k. You’ll do whatever you have to do.
But that’s the wrong question. We should be asking: How do we strike and maintain a balance to ensure we get the innovation we need at prices we can afford?
While Patients For Affordable Drugs Now would have gone further in the Inflation Reduction Act, it clearly was built with striking that balance as a foundational principle. That point is driven home by a fact that is worthy of repeating: The IRA does not change the key way our nation rewards investment and risk-taking for innovation–we continue to allow drug companies to set launch prices and maintain those prices for a minimum of 9 to 13 years before potentially facing negotiated prices.
This story from Cheryl in Louisville captures so well the challenges patients face and the need to lower drug prices. Cheryl writes: “All my inhalers, like Trelegy, are such a high cost, I do without until I have a bad episode. These inhalers cost from $350 to $800 a month. This is crazy just to be able to breathe every day. Something is wrong here.”
Cheryl is right. I feel incredibly grateful to spend my retirement fighting to fix what’s wrong so that people like Cheryl can one day enjoy theirs. We must protect the Inflation Reduction Act from being weakened. And we must move ahead with patent and PBM reforms to make our system work better for the people it is supposed to serve with lower prescription drug prices for all.
Thank you.
| AUGUSTA — Patient advocate Sabrina Fuhrer will testify today in front of the Maine state legislature’s Joint Standing Committee on Health Coverage, Insurance and Financial Services in favor of LD 1636, a bill that would lower the price of medications for Mainers. Right now, Americans pay nearly 4 times more for brand-name prescription drugs than other wealthy countries. Led by Maine Senator Ned Claxton, LD 1636, An Act To Reduce Prescription Drug Costs by Using International Pricing, would curb pharmaceutical price gouging in Maine by tying drug prices to prices in Canada. Patient advocate Sabrina Fuhrer, who lives in Old Town, will share her testimony about her 9-year-old son, Dakota, who lives with type 1 diabetes and relies on insulin to survive. Humalog, the type of insulin that Dakota is prescribed, is priced at $649.99 for a one month supply compared to Canada where the same amount is priced at $60. “Patients in America pay more for prescription drugs than anywhere else in the world,” Sabrina, who is a frontline COVID-19 screener, will say to the committee. “In Canada, a vial of my son’s insulin costs less than $50. If I could obtain that price, I’d save hundreds of dollars a month and have so much peace of mind. Bringing prices for Mainers in line with what Canada pays would provide relief to so many families like mine who are struggling to make ends meet.” In Maine, almost 1 in 3 adults have cut pills in half, skipped does, or rationed medications. Last year, Mainers paid over $170 million more on just 25 drugs, with the highest cost increases compared to the previous year. “We need change,” Sabrina will conclude. “I urge you to support LD 1636 to protect my family, my patients, and fellow Mainers from the burden of high drug prices.” An Act To Reduce Prescription Drug Costs by Using International Pricing would lower drug prices for Mainers by: |
| LD 1636 builds on P4ADNow’s previous work in Maine including the passage of the state’s drug affordability board (LD 1499) and importation program (LD 1272) in 2019. In the 2021 session, Sabrina testified in support of legislation to create an insulin safety net program (LD 673) and a price transparency measure (LD 686). Both bills are now law. The hearing and Sabrina’s testimony can be watched here today at 10:00 AM ET. Written testimony is available upon request. Following the hearing, the bill will be considered as part of the committee’s work session. |
| ### |
WASHINGTON, D.C. — Patients For Affordable Drugs founder David Mitchell will tell his story of living with incurable blood cancer and will debunk Big Pharma’s claim that patients won’t get innovative drugs without paying high prices at a 10:00 AM hearing today on rising drug prices.
Read his full testimony here.
Mitchell’s testimony will highlight stories of patients skipping doses and going into debt to afford rising prescription drug prices. And he’ll focus on the fact that right now, nearly 1 in 3 adults report not taking their medicines as prescribed because of the cost. He’ll also discuss three legislative solutions to fix our broken system:
Key Points From Mitchell’s Testimony:
Patients For Affordable Drugs is a national patient organization focused exclusively on policies to lower prescription drug prices. We amplify the voices of Americans struggling under crushing drug prices to make policymakers and elected officials see the heavy toll of high-priced drugs. Patients For Affordable Drugs does not accept contributions from any organizations that profit from the development or distribution of prescription drugs.
###
WASHINGTON, D.C. — On Tuesday, May 7 at 10:00 AM, Patients For Affordable Drugs Founder David Mitchell will testify before the Senate Judiciary Committee during a hearing on rising prescription drug prices.
Mitchell will discuss his journey as a patient with incurable blood cancer and will offer a number of solutions to lower drug prices. He will encourage bipartisan action to address this issue, including reforming the country’s patent laws, ending the days of monopoly pricing power without taxpayer negotiations, and forcing transparency from drug middlemen.
WHAT: Full Senate Judiciary Committee Hearing, “Intellectual Property and the Price of Prescription Drugs: Balancing Innovation and Competition”
WHEN: Tuesday, May 7 at 10:00 AM
WHERE: Dirksen Senate Office Building 226, or watch online
WITNESSES:
Joshua D. Barker, Director of the South Carolina Department of Health and Human Services
David Mitchell, President and Founder of Patients For Affordable Drugs
James Stansel, Executive Vice President and General Counsel of the Pharmaceutical Research and Manufacturers of America
Michael Carrier, Professor of law at Rutgers Law School
David S. Olson, Associate Professor at Boston College Law School
###
AUGUSTA, Maine — Maine patients will urge legislators to hold drug corporations accountable for exorbitant price hikes and give the state power to negotiate lower prices during hearings today and Wednesday before the Health Coverage, Insurance and Financial Services Committee. Patients For Affordable Drugs Now, a Washington, D.C.-based bipartisan patient advocacy organization that takes no money from the pharmaceutical industry, is helping patients share their drug pricing stories in Maine, sending four patients to testify at this week’s hearings on a package of bills to lower prescription drug prices. Patients For Affordable Drugs Now also published a series of patient stories on its website to underscore the urgency of the drug pricing crisis in Maine.
“Drug corporations have a direct line into Maine’s state coffers and patients’ pockets, and it’s time for the legislature to act,” said Ben Wakana, Executive Director of Patients For Affordable Drugs Now. “We’ve heard from nearly 250 Mainers who are suffering under relentless prescription drug price hikes. We applaud consumer groups and the state legislature’s efforts to rein in drug prices, and we are proud patients are standing up against abusive pricing practices.”
Here’s how the pending legislation would benefit Mainers:
Testifying at the hearings today and Wednesday are:
Lori Dumont of Brewer: “My brother suffered ketoacidosis because he could not afford his insulin. Like so many others, his insulin costs were out of control. For both his long term and short term insulin he was paying about $1,500 a month. On a fixed income, high drug prices are literally a matter of life and death.”
Sabrina Burbeck of Old Town: “When my youngest son was 18 months old he was diagnosed with Type 1 diabetes. In order to survive, he relies on Humalog Insulin. One vial of Humalog costs $350.”
Glenda Smith of Kennebunk: “My Symbicort, Lostatin, Spiriva, and other medications cost me more than $1,200/month, not to mention the $5,000 we have to pay out of pocket before insurance even begins to pay its portion. That is not realistic on our fixed income. My drug costs alone are more than my entire Social Security check.”
Christina Raymond of Limestone: “In order to manage my disease, I require several medications –– Lupron, Tamoxifen, and Neulasta –– in addition to my regular chemo treatments. Lupron costs me $1,500 per month and my Neulasta runs $6,000 per shot.”
###
BOSTON — Massachusetts patients will speak out against high drug prices tomorrow during testimony in favor of sweeping state reforms that would require drug corporations to justify exorbitant prices and give the state negotiation power on behalf of patients and taxpayers. Patients For Affordable Drugs Now, a Washington, DC-based bipartisan patient advocacy organization that takes no money from the pharmaceutical industry, is helping patients share their drug pricing stories in Massachusetts, sending two patients to testify before the Joint Committee on Health Care Financing tomorrow and publishing a raft of patient stories on its website to underscore the urgency of the drug pricing crisis in Massachusetts.
“Drug corporations have a direct line into Massachusetts’ state coffers and patients’ pockets, and it’s time for the legislature to act,” said David Mitchell, a cancer patient and the founder of Patients For Affordable Drugs Now. “We’ve heard from 265 Bay staters who are suffering under relentless prescription drug price hikes. We applaud Gov. Baker, consumer groups, and the state legislature’s efforts to rein in drug prices, and we are proud patients are standing up against abusive pricing practices.”
HB 1133 and SB 706 would:
Testifying at tomorrow’s hearing are:
Mary Mack of Nantucket: Mary lives with advanced heart failure due to a rare type of genetic muscular dystrophy. The symptoms of her disease—fatigue and shortness of breath—make it difficult to accomplish even the simplest task. Mary was on Entresto for only five months when the copay went up to $225 a month. The expense became too much for her family, so she stopped taking the drug.
Helen Fonseca of Tewksbury: Helen faces Crohn’s Disease. She plans to tell lawmakers: “I take Apriso. Before I retired, this drug cost $60 for a three-month supply. However, once I retired three years ago, the cost skyrocketed, going up to $500 for the same supply. There is no generic for this drug, even though its patent has run out. This cost is absurd. And for people like me who are on a fixed income, this cost is often impossible to pay.”
MORE PATIENT PERSPECTIVES:
Kathleen Rider, Otis, MA: “I am on a fixed income and am forced to shell out $145 for the medication every three months. It adds up. The stress of having such a costly medicine does affect my mental health. This is a necessary medication for me.”
Diane Sarmento, Lowell, MA: “I am a Medicare patient who was prescribed Ampyra, which is meant to strengthen my muscles and improve my overall quality of life. But the price of this drug is prohibitive: when I can’t get assistance, I can’t afford it.”
John Wood, West Springfield, MA: “I have type 2 diabetes that I work to keep at bay by living a healthy lifestyle. However, I also take Onglyza to help maintain my A1C levels. I usually fall into the Medicare donut hole within 6 months, causing a coverage gap. That’s when the price skyrockets to upwards of $450.”
According to recent polling from the Kaiser Family Foundation, only 25 percent of Americans say they trust drug corporations to price their products fairly. Nearly one in four Americans report difficulty affording their prescription medications.
###
WASHINGTON, D.C. — Big Pharma’s price hikes are under the microscope of the Senate Aging Committee this week with a hearing featuring patients hurt by the skyrocketing costs of their medicines.
“This hearing in the United States Senate Special Committee on Aging Wednesday will be dedicated to the testimony of patients,” said David Mitchell, a cancer patient and the founder of Patients For Affordable Drugs. “Patients are sharing their stories and leading the fight to lower prescription drug prices. We are grateful Congress is listening. More importantly, millions of Americans are depending on Congress to move quickly to action.”
For patient interviews, contact [email protected].
Patient perspectives:
Among those testifying Tuesday are Pam Holt, a retired teacher from Granger, IN and Sheldon Armus, a retiree from Boynton Beach, FL. The Medicare beneficiaries rely on expensive medications to survive.
Holt needs a cancer drug priced at $250,000 per year.
“On Medicare Part D, I went into and out of the donut hole in January — paying $4,950 the first month and then $640 for Revlimid every 28 days for the rest of the year. That cost was unaffordable for me and after just one year, it sent me into debt quickly. I was entirely underwater, and I made the heartbreaking decision to refinance my house,” Holt will tell the Senate Aging Committee.
Of the blood thinner he needs, Xarelto, Armus plans to say:
“Xarelto is one of my drugs; it is a blood-thinner that prevents dangerous blood clots that can lead to heart attacks. It is a new and expensive drug with a list price of more than $450 for a 30 day supply! It is outrageous. You’ve probably heard of Xarelto because it is heavily advertised to consumers on TV. Janssen Pharmaceuticals, the company that makes Xarelto, has promised to start disclosing the list price of its medications on those ads.
But that wouldn’t make a difference for patients like me. There isn’t a generic on the market I could turn to instead.”
U.S. patients and taxpayers spend more than $450 billion each year on prescription drugs, by some estimates, nearly one-fifth of all health care costs. Patent-protected brand-name drugs drive spending, making up only about 10 percent of prescriptions but accounting for three-quarters of drug spending.
###