By Tomi Fadeyi-Jones, Chuck Hurley, Gloria Johnson-Cusack, Cal LaRoche, David Mitchell, Nicole Solomon-Mitchell
As Democrats and Republicans consider how to deliver on their promises to lower drug prices made during the 2020 election, there’s an important imperative for reform that has gone underreported: High drug prices contribute to poor health outcomes and disproportionately harm Black and Brown Americans — perpetuating systemic racism in health care.
Racial disparities in health care are well-documented, as Black Americans are more likely to suffer from chronic pain, diabetes, high blood pressure, and COVID-19 due to economic, political, and social conditions. They are almost twice as likely to be uninsured and have lower incomes, putting a source of regular care and medical treatments out of reach for too many. As a result, the life expectancy of a Black man in America is almost five years less than that of a white man.
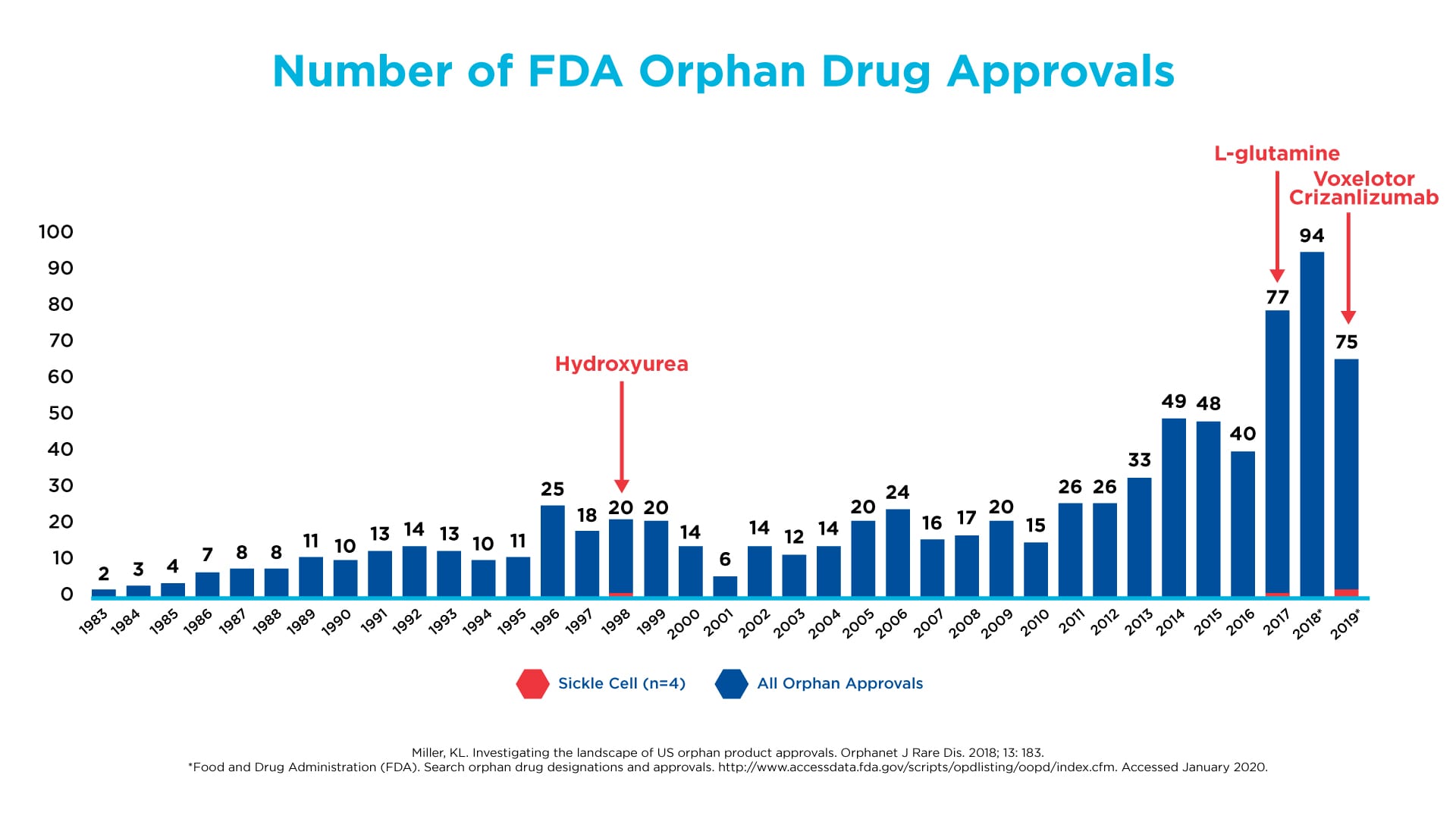
Diseases that disproportionately affect Black Americans are often under-researched by drug corporations. Sickle cell disease is a clear example. It was discovered more than 100 years ago and its cause has been understood for about 50 years, but investment and innovation have lagged far behind other drugs that treat smaller populations.
{kind=link}
Most recently, the coronavirus pandemic has brought into painful and stark view the impact of continued systemic racism in U.S. health care. Not only are Black and Brown Americans more likely to contract the virus, they are more likely to die as a result. Yet drug corporations are actively raising prices on drugs, such as anticoagulants and cardiovascular medications, that can help treat underlying conditions that may contribute to increased mortality.
The barriers to and rationing of treatment resulting from high prescription drug prices are an integral part of how systemic racism plays out in health care. By consistently putting profit maximization ahead of public health, drug companies inflict the greatest pain on those who are most vulnerable — Black Americans and other people of color. While 25 percent of white Americans report not taking prescription medications as prescribed due to cost, the number rises to 30 percent among Black Americans and 42 percent among Hispanics.
Drug corporations tout so-called patient assistance programs as a solution for people who cannot afford their drugs. But 97 percent of these programs exclude people who don’t have insurance. Why? Because these programs are really about selling more drugs at high prices; drug companies want to spend patient assistance money to cover patient copayments in order to leverage the much higher total insurance payment for a drug. Since Black Americans are almost twice as likely to be uninsured, these programs are frequently of no help to them. Those without insurance are often condemned to pay the high list prices set by drug corporations — not the discounted prices that insurers negotiate for their customers.
Yet, there is a more insidious and far-reaching impact of our drug pricing system in perpetrating systemic racism: We permit drug corporations to dictate whatever price they choose, and as a result, they extract an unearned and disproportionate share of the nation’s resources. For every dollar of taxpayer money we send to drug corporations in unwarranted profits through Medicare and other public programs, that is a dollar we don’t have to provide insurance coverage, improve nutrition, clean up water, increase funding for education, and generally support the steps that can lead to a healthier and higher quality of life for communities of color.
The bottom line with prescription drug pricing in America is that brand drug corporations insist on unfettered power to set prices as high as they choose, and diverse communities are disproportionately hurt by their practices.
We can fix our drug pricing system to make Black and Brown lives healthier and longer. To do that, there must be access to affordable prescription drugs — and that starts with lower list prices. Legislation that advanced in the U.S. House and Senate last year — most notably H.R. 3 — would move us in the right direction. It would lower drug prices in both public and private sector plans and reconfigure Medicare benefits to reduce out-of-pocket costs.
Black Americans are consistently underrepresented in clinical trials for diseases ranging from diabetes to heart disease to cancers, despite being disproportionately affected by many of them. H.R. 3 included more money for the National Institutes of Health; we believe a greater share of that funding should be earmarked for conditions that disproportionately affect people of color and to fund clinical trials that include representation of all Americans.
At the state level, the NAACP has endorsed the creation of drug affordability boards “to determine how best to make prescription drugs more affordable for residents,” and we are working in support of legislation to establish boards in several states.
The late Congressman Elijah Cummings summed it up clearly a few years back and made this link to high drug prices: “These factors place African Americans in a double bind — we are more likely to suffer from an expensive chronic disease and we earn less money with which to pay for our health care, including skyrocketing prescription drug prices.”
Black lives matter. We remain committed to and will continue the fight for reform, and a new healthcare system that prioritizes public health — especially the health of Black Americans and all people of color — over unjustified profits for multinational drug corporations.
###
The authors are members of the Boards of Directors of Patients For Affordable Drugs and Patients For Affordable Drugs Now.