WASHINGTON, D.C. —An insidious culture of greed is pervasive across the pharmaceutical industry, and today the scale of the problem was revealed. The House Oversight Committee’s investigation into drug corporations exposed a disturbing pattern of abusive pricing practices, anti-competitive behavior, and manipulative marketing campaigns.
Not a single price increase was linked to investment in research and development, according to the documents. Instead, drug corporations took unrelenting price increases to meet revenue goals, increase executive bonuses, and maximize corporate profits.
The reports examine Amgen, Novartis, and Mallinckrodt and reveal the falsehoods behind pharma’s favorite talking points.
Read highlights from the damning documents below.
1. Pharma Claim: High prices exist to recoup R&D, not drive profits.
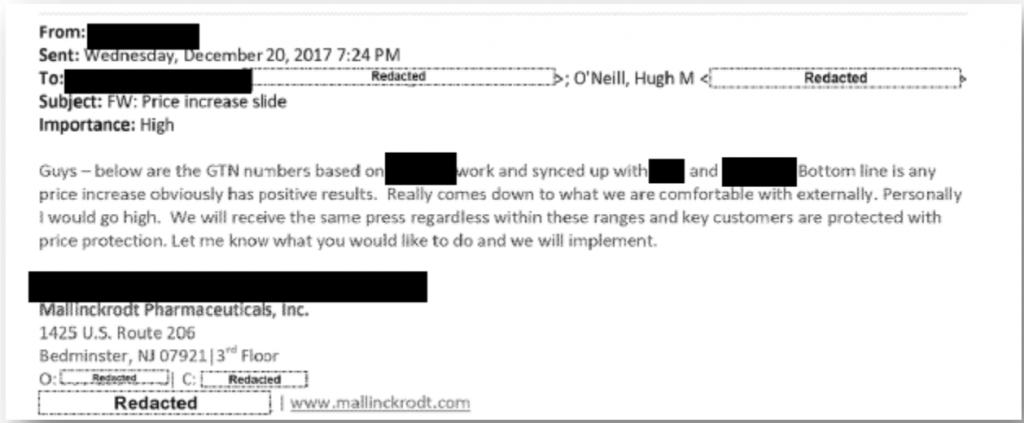
The reality: Executives’ motivations for price hikes is devoid of desire to recoup or invest in R&D — instead the hikes are intended to increase revenue. Internal company documents showed that company executives weighed price increases against public backlash, not the actual impact on research and development funds. Ultimately, executives decided in favor of price hikes because “we will receive the same press regardless” and “any price increase obviously has positive results.”
2. Pharma Claim: We make life-saving drugs — it’s not about the money for us.
The reality: The committee’s investigation found that executive compensation policies incentivized price hikes. Novartis increased the price of Gleevec 22 times, and its revenue soared. As a result, more than 100 Novartis employees made $1 million in 2014 and 2015.

3. Pharma Claim: Our decision-making centers on the health and well-being of patients.
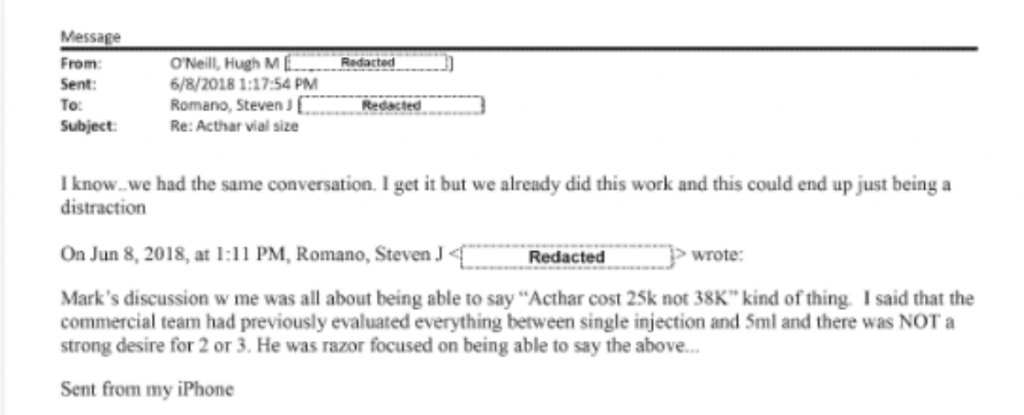
The reality: After public outrage at its $40,000 price for a single vial of Acthar Gel, Mallinckrodt’s CEO urged changing the vial size of Acthar gel (nearly cutting it in half) to appear like the company decreased the price.
4. Pharma Claim: Charity programs ensure our drugs are affordable and accessible.
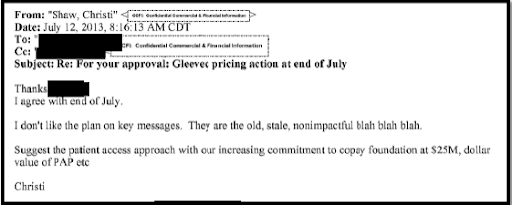
The reality: Patient assistance programs serve both as a public relations tool for companies and to increase their bottom line. Novartis’ internal strategy documents estimated the rate of return of its co-pay assistance program would be $8.90 for every dollar invested. When weighing “key messages” to employ after a highly scrutinized price hike, one Novartis executive urged colleagues to emphasize contributions to the copay foundation.
5. Pharma Claim: It’s a robust marketplace and drug companies compete based on price.
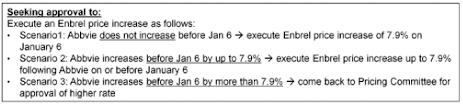
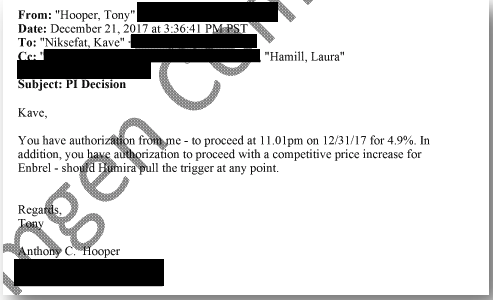
The reality: Drug companies often collude — not compete. Amgen’s business strategy for its blockbuster Enbrel centered on matching price hikes by its biggest competitor, AbbVie’s Humira. Internal presentations reveal that Amgen planned its price hikes based on the behavior the company anticipated from AbbVie.
6. Pharma Claim: High prices fuel innovation.
The reality: Taxpayer funding fuels innovative new drugs. High prices fuel the growth of Big Pharma revenue. Drug companies don’t invest until public research shows commercial promise.

7. Pharma Claim: Pharmacy benefit managers are responsible for price increases.
The reality: Big Pharma loves to point fingers, but internal documents show price increases on Amgen’s Enbrel and Sensipar are unrelated to rebates negotiated with PBMs. Instead, the price hikes are used to raise the company’s revenue.
Read our takeaways from yesterday’s reports from the House Oversight Committee into pharma giants Celgene and Teva.
###
By Sarah Kaminer Bourland, Legislative Director
1. Pharma Claim: High prices exist to recoup R&D, not drive profits.
The reality: Executives’ motivations for price hikes is devoid of desire to recoup or invest in R&D — instead the hikes are intended to increase revenue. Internal company documents showed that company executives weighed price increases against public backlash, not the actual impact on research and development funds. Ultimately, executives decided in favor of price hikes because “we will receive the same press regardless” and “any price increase obviously has positive results.”
2. Pharma Claim: We make life-saving drugs — it’s not about the money for us.
The reality: The committee’s investigation found that executive compensation policies incentivized price hikes. Novartis increased the price of Gleevec 22 times, and its revenue soared. As a result, more than 100 Novartis employees made $1 million in 2014 and 2015.
3. Pharma Claim: Our decision-making centers on the health and well-being of patients.
The reality: After public outrage at its $40,000 price for a single vial of Acthar Gel, Mallinckrodt’s CEO urged changing the vial size of Acthar gel (nearly cutting it in half) to appear like the company decreased the price.
4. Pharma Claim: Charity programs ensure our drugs are affordable and accessible.
The reality: Patient assistance programs serve both as a public relations tool for companies and to increase their bottom line. Novartis’ internal strategy documents estimated the rate of return of its co-pay assistance program would be $8.90 for every dollar invested. When weighing “key messages” to employ after a highly scrutinized price hike, one Novartis executive urged colleagues to emphasize contributions to the copay foundation.
5. Pharma Claim: It’s a robust marketplace and drug companies compete based on price.
The reality: Drug companies often collude — not compete. Amgen’s business strategy for its blockbuster Enbrel centered on matching price hikes by its biggest competitor, AbbVie’s Humira. Internal presentations reveal that Amgen planned its price hikes based on the behavior the company anticipated from AbbVie.
6. Pharma Claim: High prices fuel innovation.
The reality: Taxpayer funding fuels innovative new drugs. High prices fuel the growth of Big Pharma revenue. Drug companies don’t invest until public research shows commercial promise.
7. Pharma Claim: Pharmacy benefit managers are responsible for price increases.
The reality: Big Pharma loves to point fingers, but internal documents show price increases on Amgen’s Enbrel and Sensipar are unrelated to rebates negotiated with PBMs. Instead, the price hikes are used to raise the company’s revenue.
###
By Sarah Kaminer Bourland, Legislative Director
1. Pharma Claim: High prices exist to recoup R&D, not drive profits.
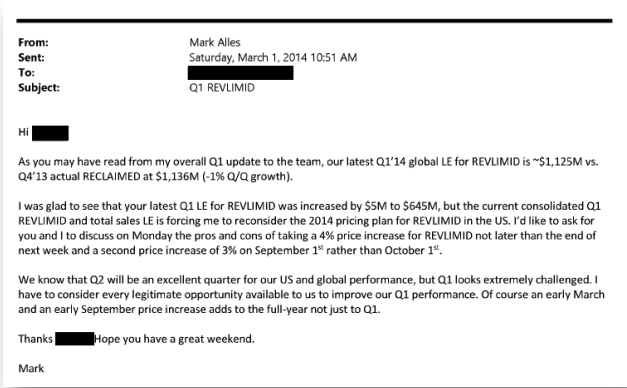
The reality: In a 2014 email from Mark Alles, Celgene’s CEO, the executive admits that he’s planning a price hike to meet sales targets. Furthermore, the investigation concluded that Celgene’s internal pricing decisions “were divorced from its calculus regarding future R&D or recouping of past R&D expenditures.”
2. Pharma Claim: We make life-saving drugs — it’s not about the money for us.
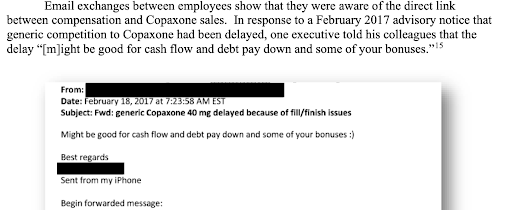
The reality: Instead of inviting a competitive market, drug companies thwart competitors at every turn. When news broke that a generic competitor had been delayed, Teva employees celebrated by exchanging emails about the financial implications for their bonuses.
3. Pharma Claim: Our decision-making centers on the safety and well-being of patients.
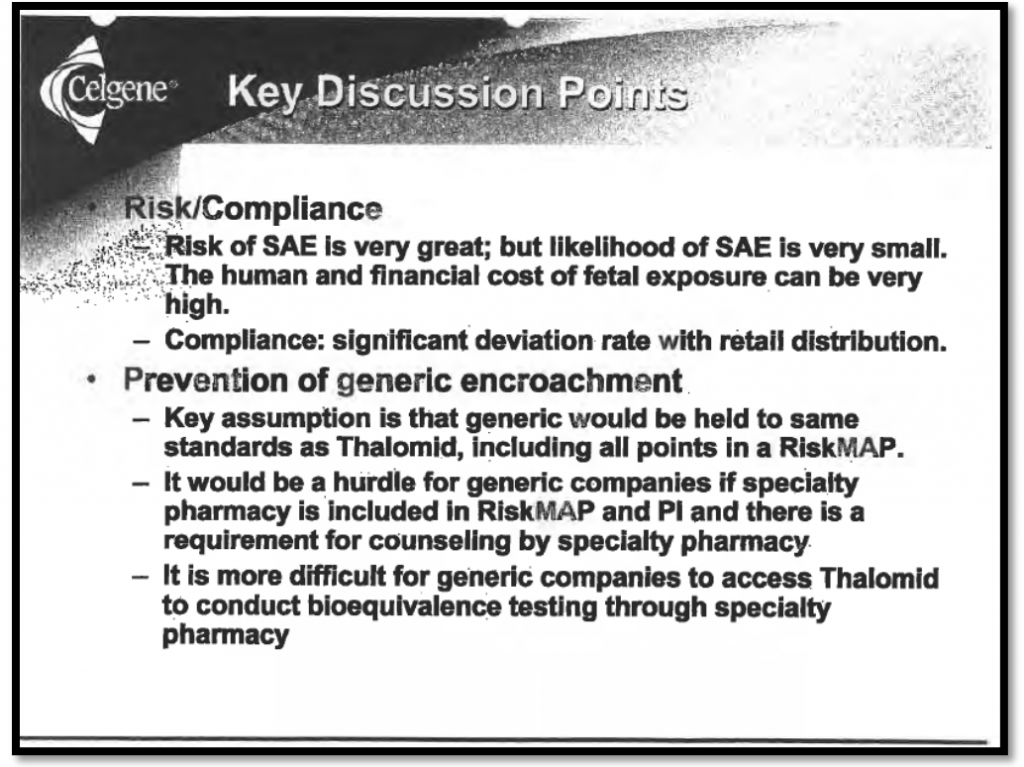
The reality: Celgene has long cited “safety” concerns as the company’s rationale for blocking generic competition through the FDA’s risk evaluation and mitigation strategies (REMS) program. But internal documents published today show that the company views their REMS program not as a means to promote safety, but as a tool to prevent “generic encroachment” and extend its monopoly.
4. Pharma Claim: Charity programs ensure our drugs are affordable and accessible.
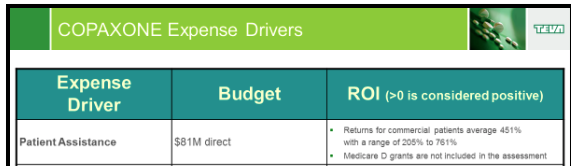
The reality: An internal presentation reveals that Teva averages a 451 percent return on every dollar invested in its copay assistance program. Teva’s program covers out-of-pocket expenses for patients while generating a full reimbursement for the drug corporation from each patient’s insurance company.
5. Pharma Claim: We support solutions to lower drug prices for patients.
The reality: Between 2017 and 2020, Teva spent $11.6 million lobbying Congress in order to thwart reforms that would harm its bottom line. According to internal documents, one of Celgene’s internal goals was to prevent the “legislative erosion” of the program it uses to prevent generics from coming to market.

6. Pharma Claim: High prices fuel new drugs.
The reality: Copaxone generated $34.2 billion in net U.S. revenue for Teva over nearly two decades. The drug corporation spent only 2 percent of that on R&D for the drug. Instead, Teva invested in developing “new” versions of old drugs that offer no therapeutic benefit.
7. Pharma Claim: Pharmacy benefit managers are responsible for price increases.
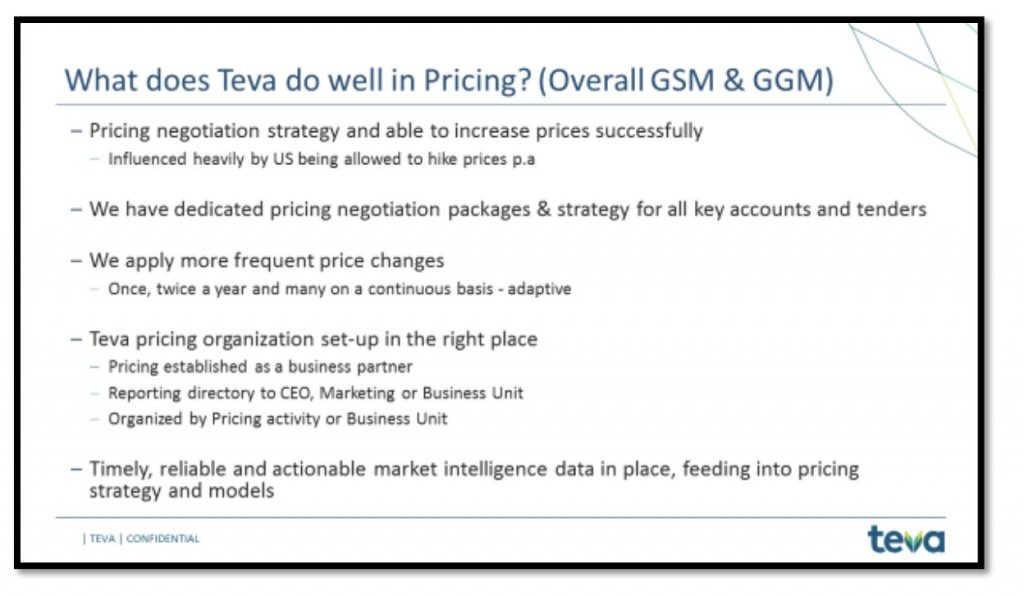
The reality: Drug companies alone set and control prices. In company PowerPoints, Teva boasted about its success increasing prices.
###
My name is Kolton Chapman and I live in Pickerington, Ohio. I am a transgender man living with a chronic illness. My life hasn’t always revolved around my illness –– I am an artist who enjoys coloring books and helping people design logos and other items to help with their businesses. I am a son who loves to spend time with his family, and I am an insurance agent. That last one is what I am most proud of. I have worked very hard to get to where I am today, and even with everything working against me, I was able to achieve my goals. I view every scar that I carry as proof that I have survived this long, and that it is going to take a lot more than that to break me.
In 2014, I was diagnosed with ulcerative colitis. After my diagnosis, I began taking Lialda to try and put my disease into remission. Just one month’s supply of that cost me $250, because there was no alternative drug available. That $250 was my cost even after what my insurance company covered. Two years in, I began receiving Entyvio infusions for my ulcerative colitis every four weeks. When I first began infusions, Entyvio was totally covered by my insurance. But I later had to change insurance coverage due to circumstances out of my control, and the price became astronomical. Every four weeks, I had to pay $1,200 per infusion under my new insurance.

At the time of this cost increase, I was in college and was already feeling the financial burden of student debt. Budgets for students are already tight enough, but the immense increase in cost for my infusions left me in an incredibly difficult position. Unfortunately with the added financial burden from my infusions, I had to choose between affording the cost of my infusions or school. This decision really wasn’t a decision at all since I needed the infusions to stay alive. The unreasonable price of my prescriptions forced me to leave college.
Because of the astronomical cost of my Entyvio infusions, I now owe more in medical debt than I do in student loans. The massive financial burden from medical and student debt factors heavily into my decisions. I had to remove my colon, knowing that it was the only thing I could do to avoid more debt. Our medical decisions shouldn’t be driven by what will protect us from the most debt, but what will bring about the best health outcomes.
In 2019, I was diagnosed with moyamoya disease, a rare blood vessel disorder, and have already suffered a stroke. My main priority through my health challenges should be focusing on my health –– not on bills and making ends meet. But unfortunately, with high prescription costs, their prices and my medical debt always factor into my decisions. Although I now have different coverage and am taking different prescriptions, I still spend over $150 per month on my four medications. This cost may seem more manageable compared to the $1,200 I was spending monthly on infusions before, but it’s still an incredible financial burden that is only being added on top of the remaining medical debt hanging over my head from earlier infusions.
My life path has been completely altered by expensive prescription drugs and drug company greed. I often feel like I’m behind all of the people my age — even people younger than me — because I’ve had to focus my time and money on staying alive. We shouldn’t have to give up on pursuing a college education because of crippling medical debt. We shouldn’t have to make every financial decision with the cost of prescriptions and medical debt in the back of our minds. Things can be better if our leaders rein in drug companies’ greed and make the needs of patients like me the priority.