Click here for a downloadable PDF with citations
Testimony of David E. Mitchell Founder, Patients For Affordable Drugs NOW before the U.S. Senate Committee on the Judiciary for a hearing on “Ensuring Affordable & Accessible Medications: Examining Competition in the Prescription Drug Market”
May 21, 2024
Chairman Durbin, Ranking Member Graham, members of the committee. Thank you for inviting me to testify today at this important hearing examining how we can lower prescription drug prices by curbing the rampant anticompetitive conduct in prescription drug markets that is hurting patients, consumers, and taxpayers across America.
Section I. Background and Introduction
My name is David Mitchell. I am the founder of Patients For Affordable Drugs NOW. We are the only national patient advocacy organization focused exclusively on policies to lower prescription drug prices. We are independent, bipartisan and we don’t accept funding from any organizations that profit from the development or distribution of prescription drugs.
Since we launched a little over seven years ago, more than 35,000 patients across all 50 states have shared stories with us of their struggles to pay high drug prices. And we have built a community of more than three-quarters of a million patients and allies supporting policies to lower drug prices.
More importantly for today, I have an incurable blood cancer, and prescription drugs are keeping me alive — literally.
My oncologists currently have me on a four-drug combination of infused and oral cancer medications. These four drugs carry a combined list price of more than $1 million per year. Just one of my oral drugs, called Pomalyst, is priced at more than $22,400 for 21 capsules, which I must buy every 28 days. And because Medicare beneficiaries like me pay our out-of-pocket costs based on list price, I spent more than $16,500 out-of-pocket last year — just for Pomalyst. To help manage the cost of my infused drugs, I spend another $3,980 per year to purchase a Part B supplement. And of course, I have the base costs of Medicare to pay as well.
But the Inflation Reduction Act has changed that equation completely. After paying more than $16,000 last year because there was no out-of-pocket maximum in Part D, I am paying only $3,326 this year as an out-of-pocket cap began to phase in. Next year, the maximum anyone on Medicare will pay annually for drugs is $2,000. Our patients who have been unfortunate enough to contract a disease or condition requiring expensive drugs are elated–they say it is life-changing. Judy from Maine wrote to us a few weeks ago saying:
“I have to admit that I was still a bit skeptical about the Medicare changes until today. In January my copay for Enbrel was $2,150.83. In February it was $1,141.86. Today it was zero. I was thrilled, as was the staff at the pharmacy.”
That’s just one story. There are many more like that.
Here on this slide is the state of my disease today. This slide below is from a presentation to the FDA’s Oncologic Drugs Advisory Committee on March 15 of this year on the state of multiple myeloma in the U.S. Please note the last point.
The last point is always sobering to reflect on: “Despite this improvement, most patients with a diagnosis of myeloma will die from the diagnosis.” Yet, I am a very lucky man — the drugs are currently keeping my cancer at bay, and I tolerate them pretty well. But with multiple myeloma, nothing works forever. This is why innovation is so important to me. And it goes to the heart of the reason for this hearing:
We rely on patents to incentivize and reward innovation. We give drug companies limited-time monopolies to charge whatever they like in order to ensure a rich reward for the development of innovative new drugs. We need that innovation. I need it personally. But drugs don’t work if people can’t afford them. And too often drug companies abuse the current patent system, not to reward innovation, but to block competition that would lower prices as the patent laws intend. The bipartisan bills that are the focus of today’s hearing aim to address that abuse and restore the intended balance.
For me personally, the point is: I need innovative new drugs. I care deeply about innovation and new drug development. My life depends on it. Without innovation, I will die sooner than I hope to. That is not a plea for sympathy–it’s just an unfortunate fact.
But my more than 13-year journey as a cancer patient has taught me that our current system which relies on competition and market forces to lower drug prices after a period of monopoly pricing is not working. I’m here to ask each of you to fix it.
Section II. The High Prices Americans Pay For Drugs and Need For Further Reforms
Drugs are too expensive in the United States. Americans pay more than four times what people in other wealthy nations pay for the exact same brand-name drugs. Even after applying estimated rebates to arrive at net prices, Americans are still paying more than three times what people in other wealthy nations pay for the same brand-name drugs.
Consequently, about three in ten Americans report having difficulty affording their medications. When their prescription drug prices are too high, Americans face challenges affording other expenses, such as food and housing. One survey found that over 20 percent of people took on debt or declared bankruptcy because of their medications.
High drug prices disproportionately harm communities of color. One in two Latinos in the United States takes a prescription medication, and more than 20 percent are uninsured. Black and Latino adults aged 65 and older were more likely to report difficulty affording prescription medications than White adults. Further, Black Americans are more likely to live with chronic pain, diabetes, and high blood pressure than white Americans and are nearly two times more likely to be uninsured.
As expensive as my drugs are, even with Medicare out-of-pocket caps taking effect, I never lose sight of the fact that roughly 26 million Americans don’t have any health insurance at all and are exposed to the full list price of the medications they need.
The reality is that people struggle to pay these high prices with and without insurance.
Americans have been demanding relief for years. A KFF poll in July of 2023 found three out of four Americans said there is not enough government intervention when it comes to limiting the price of prescription drugs. That includes 82 percent of Democrats, 67 percent of Independents, and 68 percent of Republicans. In the wake of the enactment of the Inflation Reduction Act which is helping millions of people by lowering prices and making drugs more affordable–Americans want more done.
Section III. The Need for Patent Reform
When a drug company makes a truly innovative discovery, it should be rewarded with a patent and receive a fair return for the risk and investment it undertook. Our patent system was created to facilitate these rewards for innovation so that drug companies are incentivized to pursue true clinical breakthroughs and inventions that bring meaningful benefits to patients.
But the drug industry would have you believe that every patent is deserved and that the sheer volume of patents granted is an appropriate indicator of innovative achievements. That couldn’t be further from the truth.
Neither new patents nor new drugs equal new innovation. Worse, in too many cases, manufacturers are abusing America’s patent and exclusivity system –not to reward innovation – but to prevent free-market competition and block affordable generic and biosimilar drugs from coming to market.
Between 2005 and 2015, 74 percent of the new drug patents issued were for drugs already on the market. A second study of the ten top-selling drugs in 2021 corroborated that number. Of the roughly 100 best-selling drugs in another study, nearly 80 percent obtained an additional patent to extend their monopoly period.
In fact, gaming of the patent system to extend monopolies beyond the time intended under law inhibits true innovation patients like me need. If big drug companies can block competition and raise prices on old drugs at will in order to drive profits and executive bonuses, they have far less incentive to take risks by investing in research and development (R&D) to develop innovative new drugs that could command high prices and save lives.
There are a variety of strategies used by drug corporations to extend monopolies, including product hopping, evergreening, patent thicketing, pay-for-delay deals, and abuse of the U.S. Food and Drug Administration (FDA)’s citizen petition process.
These tactics lead to longer exclusivity than our laws intend. The median length of post-approval market exclusivity for small-molecule drugs in one study was not five years or even the seven years allowed for orphan drugs. Instead, it was 12.4 years.
Product Hopping
Let’s start with product hopping. This tactic occurs when a brand-name company switches a patient population from an older product whose patent is coming to an end and facing imminent competition to a different formulation that has a later expiring patent and therefore, is not facing competition. The “new” drug typically offers little or no new clinical benefit, it may even be as simple as changing a product from a tablet to a capsule.
This switching takes two forms. In “hard” switches, the brand-name company removes the older product from the market, forcing patients onto the new version. With “soft” switches, the company keeps the older product on the market, but engages in aggressive marketing to prescribers and patients, urging them to switch to the newer formulation. By switching their market to a “new drug,” brand-name companies effectively eliminate the market for new generics that rely on automatic substitution state laws to gain traction in the patient populations.
As patients, we support product evolution that improves effectiveness or reduces toxicities of a drug. I take a drug that causes painful peripheral neuropathy—loss of feeling in my feet. If a reformulated drug were to reduce this type of side effect, it might well meet an appropriate standard for an innovative change meriting a patent extension.
Unfortunately, this is often not the case for patients. Two drugs that have been involved in high-profile product hopping cases are Suboxone and Tricor, which treat opioid dependence and high cholesterol respectively. Here’s what patients have told us about both:
Samantha from West Virginia writes:
“I have been in recovery for over ten years now. The cost of Suboxone is outrageous — especially since, from the time I began taking it until now, the price is still as high or higher. It’s ridiculous! It’s easier for people to misuse narcotics (the cost is less). The cost for Suboxone is about $800 [for a 90-day supply].”
Beatel from Minnesota told us:
“When I changed to Medicare at 65, my price for 40mg of Tricor went to $1,800/month. The pharmacist whispered to me, ‘If the doctor changed the order to 160 mg tabs and I broke it in half for the 80 mg dose, it would cost me $40.’ The drug company still had the patent on the 40mg tab. The patent for the 160mg tab had expired…same drug.”
Patent Thickets
Patent thicketing is a tactic similarly designed to undermine market competition at the expense of patients. This strategy occurs when drug companies file dozens of non-innovative patents in order to create an impenetrable “thicket” around a drug product forcing a prospective generic or biosimilar competitor to litigate through each of the patents in order to gain market entry.
Let’s look at another drug I take to prevent blood clots and stroke–Eliquis. In 2021, it was the most expensive drug for Medicare at $12.6 billion. Its maker-Bristol Myers Squibb (BMS) has applied for 48 patents and been granted 27, blocking competition in this country for 40 years. The list price for a 30-day supply in the U.S. is about $600. The cost in Canada–where there is a generic on the market–is less than $75.
The encouraging news is that there are multiple bills before the Senate designed to close loopholes in our patent system that are harming patients. All have bipartisan support. Many have already cleared this committee on strong bipartisan votes.
● P4ADNOW supports S. 150, the “Affordable Prescriptions for Patients Act of 2023,” which cracks down on patent thickets in the biologic market and is projected to save hundreds of millions of dollars. There is also a new bipartisan bill-S. 3583-which has not cleared committee and we support that bill as well.
● S. 150 also addresses product hopping. When combined with the legislation’s patent thicket provisions, the bill could save $1 billion.
● Pay-for-delay continues to be a problem, despite the Actavis decision. This tactic occurs when brand-name drug companies provide something of value to a potential competitor to induce them to delay selling a generic version of a drug, therefore keeping it off the market in order for the brand-name drug to maintain a monopoly for longer. P4ADNOW has endorsed S. 142, a bipartisan bill to curb pay-for-delay agreements that the nonpartisan Congressional Budget Office (CBO) estimates could save $600 million.
● The citizen petition process at the FDA was designed so that patients could raise safety concerns about drug approvals. But research has revealed that the citizen petition process has been co-opted by corporations looking to block competition. Brand-name drug makers were behind 92 percent of all citizen petitions filed between 2011 and 2015. But they were not raising legitimate safety concerns, which is why the FDA threw out nine of every 10 of the industry’s “sham” petitions, which were without scientific merit and filed for the sole purpose of delaying generic competition, keeping prices high for patients. P4ADNOW supports both S. 148 and S. 1067 which will reform this process, promote generic competition, and save millions of dollars.
● Current FDA policies prohibit the agency from disclosing information generic companies need in order to speed approval of new generic competitors. P4ADNOW supports S. 775 which will increase transparency and facilitate generic entry. This bill is projected to save more than $800 million.
● P4ADNOW also supports S. 79 which will establish a task force between the United States Patent and Trademark Office (USPTO) and FDA in order to improve communication in the implementation of each agency’s patent-related activities.
- P4ADNOW also supports the bipartisan bill S. 1250 – the Drug-price Transparency for Consumers Act of 2023- which is led by Chairman Durbin and Senator Grassley, and supported by Senators from both sides of the aisle. It will provide useful information to consumers by including prices on prescription drug advertising. And don’t fall for the “no one pays list” argument against the bill; two-thirds of Americans pay for some or all of their out-of-pocket costs based on list price. List price matters greatly to us.
To achieve true innovation at prices that are affordable over the long haul, we must reform our patent and exclusivity system so that it is once again focused on driving innovation that saves lives, not driving high prices that make lifesaving drugs unaffordable to those whose lives depend on them.
Section IV. What Else Should We Do? Reform Pharmacy Benefit Managers (PBMs)
While the headwaters of our drug pricing problems are the list prices set by drug corporations, there are other reforms needed downstream in the supply chain. Pharmacy benefit managers (PBMs) are black boxes that cut secret, mutually beneficial rebate deals with manufacturers, and none of it is transparent. We need to increase transparency and curb anticompetitive practices by PBMs.
It is simply wrong that patients like me don’t know if the preferred drug on a PBM formulary is there because it is the best drug, because it is the least expensive drug among equally effective options, or because the PBM got a big, legal kickback from the manufacturer. Without transparency, it is impossible to know how much of a rebate is going to the PBM, to the insurer, to lower my premiums, or to reduce my out-of-pocket costs at the pharmacy counter. With the Big Three PBMs–Cigna, Optum Rx, and CVS Health–in control of 80 percent of the $633 billion in U.S. spending on drugs, that is more than half a trillion dollars flowing through just those three entities annually., And vertical integration uniting all three major PBMs with insurers only increases their market power. Opaque practices with that kind of money involved are a bad way to run a railroad. It’s time for transparency to ensure PBMs are operating in the best interests of patients and consumers.
It’s not just about transparency either. Drug companies and PBMs also enter into rebate arrangements that are designed to thwart lower-cost competition. These are commonly called “rebate walls,” defined as:
“Exclusionary contracting practices that a drug manufacturer deploys to limit the ability of rivals from gaining preferred access to the formulary, or any access at all. Branded manufacturers leverage their position as market leaders by offering financial incentives to pharmacy benefit managers and health insurers in the form of ‘all or nothing’ conditional volume-based rebates, in exchange for virtually exclusive positioning on the formulary. …If the payer does not accept the rebate agreement for a particular indication, it may lose all rebates for its product on all covered indications.”
Let’s be clear: These rebate deals are designed to benefit both the manufacturer seeking to block competition and the PBM that gets a bigger rebate. These deals are not designed to help patients like me by lowering prices or increasing patient choice. They are emblematic of our drug pricing system which has been built to benefit those who profit from it at the expense of those it is supposed to serve.
P4ADNOW supports reforming the practices of PBMs, including transparency requirements in order to determine how rebates are actually working — how much is going to reduce premiums and out-of-pocket for patients and consumers and how much is going to increase profits for the PBMs or insurer plan managers. In our ideal world, PBMs would have a fiduciary responsibility to patients and all beneficiaries, and all reforms would put patients at the center. While none of the PBM bills go as far as we would like, each takes important steps in the right direction and would make meaningful and important progress in the regulation and oversight of PBMs. We support key provisions of bills that have cleared the Finance Committee on unanimous or near-unanimous bipartisan votes:
- Modernizing and Ensuring PBM Accountability Act – S. 2973. We especially support the transparency and disclosure requirements, and the provisions de-linking PBM compensation from prices.
- Better Mental Health Care, Lower-Cost Drugs, and Extenders Act – S 3430. We think the required reports to Congress are of particular importance. We support the concept of the rebate pass-through provisions, but we need to see CBO scoring for this provision, and we are concerned about the impact on premiums.
The House Energy and Commerce Committee has also advanced legislation addressing PBM practices. We support provisions in the Lower Cost, More Transparency Act, H.R. 5378, that improve transparency and reporting requirements. We were also pleased to see the House Ways and Means Committee include reform delinking PBM compensation from prices in legislation it advanced earlier this month – H.R. 8261, the “Preserving Telehealth, Hospital, and Ambulance Access Act. In our view, however, none of the provisions in House legislation go far enough in reforming PBMs and ensuring they are putting patients and consumers first.
We are also following closely and supporting the Federal Trade Commission (FTC) investigation into PBMs as well. We look forward to the first interim report on that investigation expected this summer. We hope Congress uses the report to inform future legislation, and that Congress gives strong backing for the FTC to take action it may recommend.
Section V. The Inflation Reduction Act Strikes A Balance To Ensure Innovation We Need At Prices We Can Better Afford
It’s important to note that the Inflation Reduction Act (IRA) is built to strike a balance to ensure the innovation we need at prices we can better afford. In the run-up to the enactment of the IRA, the drug industry kept telling us that the legislation would stifle investment and kill innovation and access to new drugs. No one cares more about innovation than patients. But if you pull back the curtain on this pharma fear-mongering and look at what has actually happened since the IRA enactment, the argument doesn’t hold up. Here are eight reasons why.
The industry has plenty of money for innovation. In the wake of the Inflation Reduction Act passage, investors are upbeat. Drug company stocks are doing fine. The industry is flush with cash and has great access to capital.
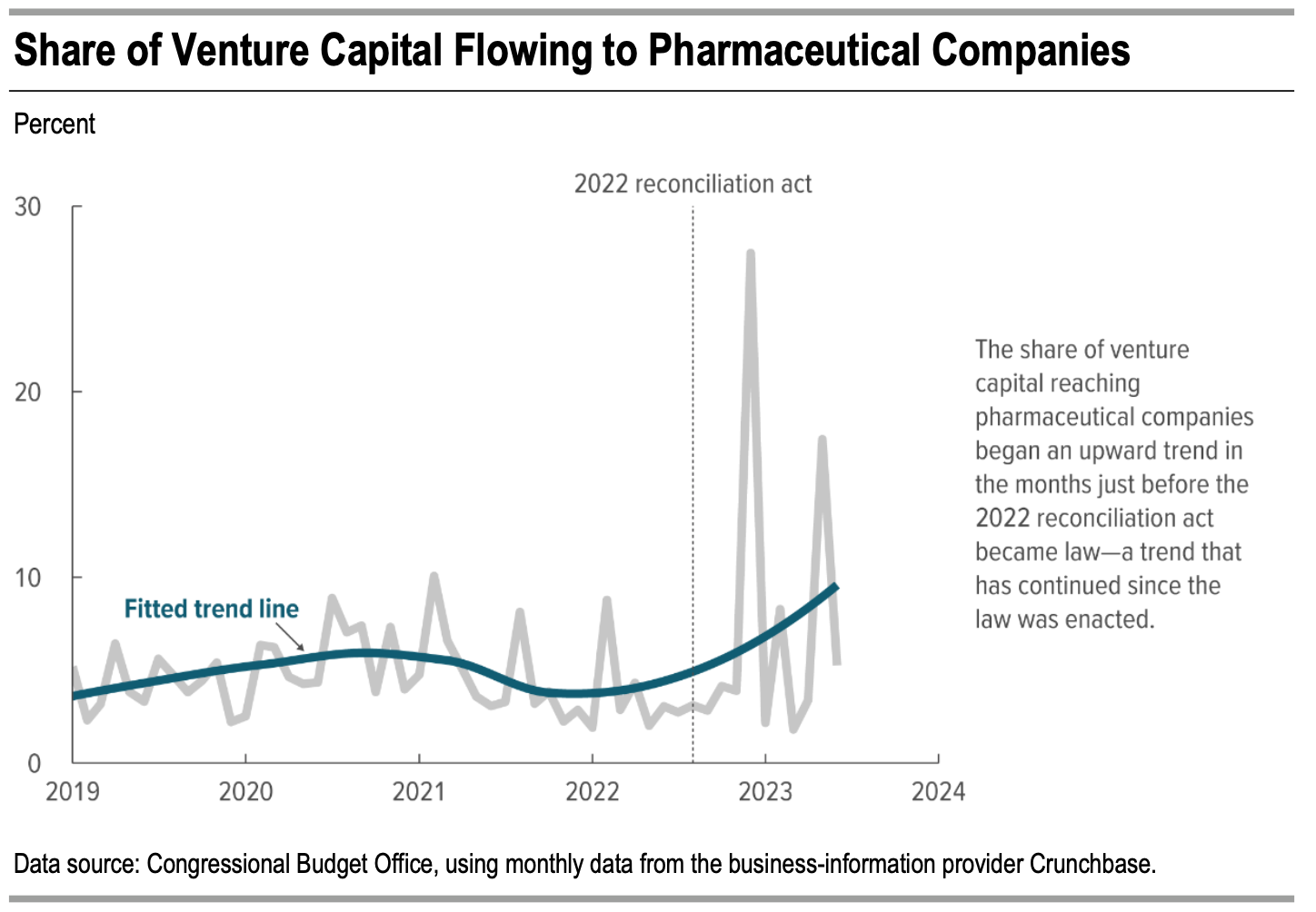
According to the Congressional Budget Office (CBO), despite Big Pharma’s claims that the implementation of the Inflation Reduction Act would stifle innovation and significantly impact profit margins, there has been a consistent and continuous increase in venture capital investment in pharmaceutical companies, demonstrating stability and resilience within this sector as shown in Figure 1.
Figure 1.
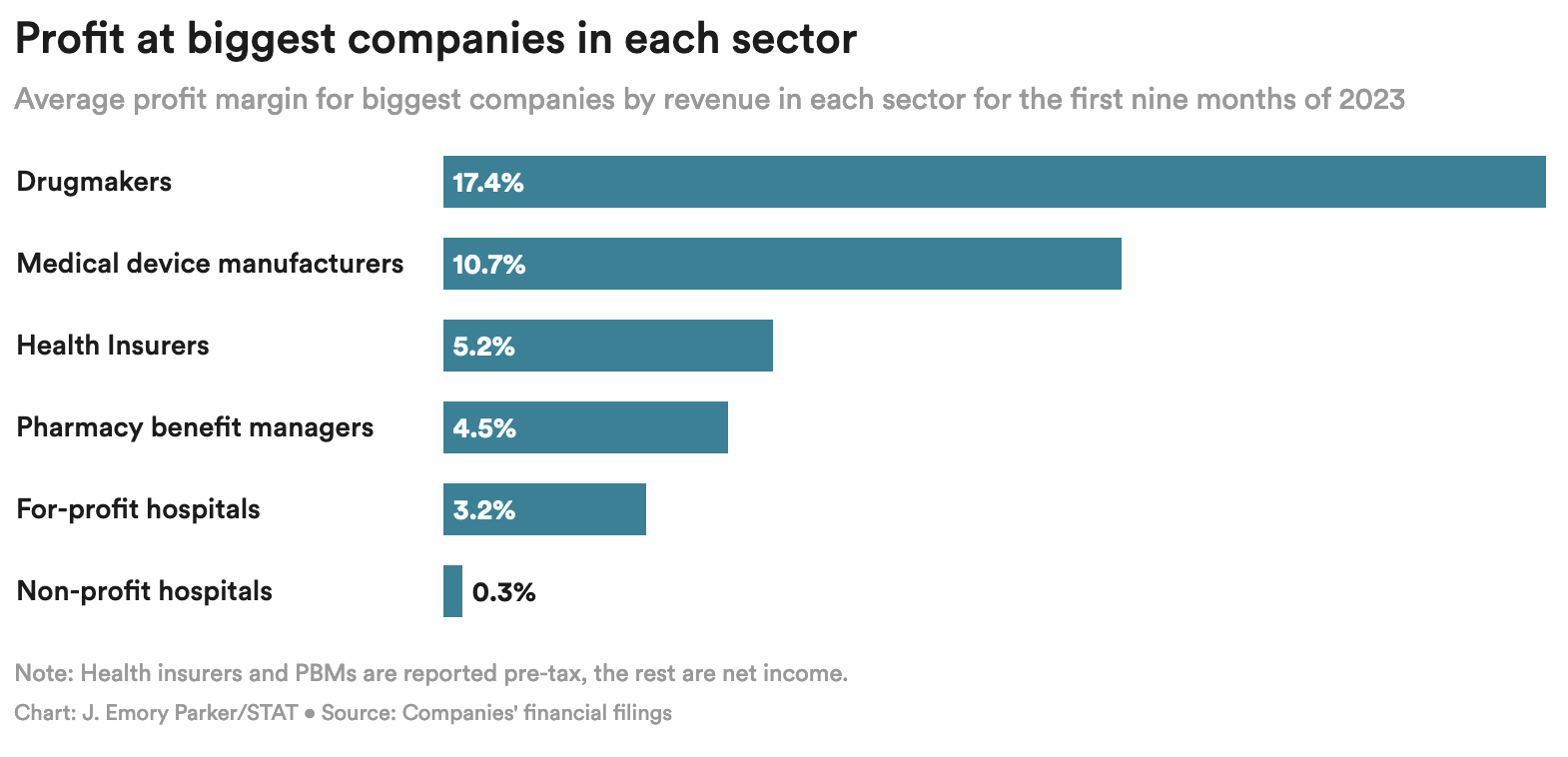
Drug companies remain by far and away the most profitable sector of the healthcare industry–more than tripling the profit of Pharmacy Benefit Managers (PBMs) and insurers.
Figure 2.
Since the passage of the Inflation Reduction Act:
- Pfizer acquired biotech company Seagen for $43 billion.
- Sanofi bought a diabetes product company for $2.9 billion.
- Novartis spent $15 billion in a stock buyback.
- Even in the face of the Inflation Reduction Act, drug companies reported increased investment in research and development (R&D). For example, in 2022 10-K filings, Johnson & Johnson reported an 11.8 percent increase in R&D spending in 2022, Merck reported an 11 percent increase in R&D spending, and Moderna reported a 65 percent increase in R&D spending and projected further increases in 2023.
- “Bayer plans to invest $1 billion on research and development this year in an effort to double its sales in the United States within a decade.”
- Sanofi said that it would increase the number of Phase 3 studies it is conducting by 50 percent between 2023 and 2025 at a financial cost of about $700 million a year.
The Inflation Reduction Act incentivizes innovation by curbing drug companies’ ability to drive profits by raising prices on old drugs at will.
- To make more money, drug companies will have to develop high-value new drugs that can command high prices, instead of repurposing old products.
- The negotiation process includes the consideration of therapeutic advances and meeting unmet needs, which will reward more innovative drugs.
- The law maintains the key incentive for innovation that currently exists in the U.S. by allowing drugmakers to be compensated handsomely for investment and risk by setting their launch prices, maintaining the Food and Drug Administration (FDA)-awarded period of exclusivity, and exempting all medications from negotiated prices for a nine to 13 year period.
- The U.S. will continue to pay the highest drug prices and offer the largest pharmaceutical market in the world. Drug companies will continue to innovate in order to have access to such a lucrative market.
The Congressional Budget Office (CBO) says the Inflation Reduction Act will have a minimal to non-existent impact on new drug development.
- According to the CBO, the Inflation Reduction Act will decrease the number of new drugs over the next 30 years by only about 15 out of 1,300 expected – that’s only a little over one percent.
- Since only 10 to 15 percent of “new” drugs represent true therapeutic advancements, of the 15 new drugs foregone, only one or two might actually be true innovations.
- Pharma cries poor every time policy reforms take even a small piece of change out of its pocket. But the reduction in drug industry revenue from the Inflation Reduction Act will be very small overall — estimated at less than one percent through 2032. Figure 3 shows we are barely making a dent in the drug industry’s global revenues with Medicare negotiation, which the industry is spending an enormous sum of money to prevent in the courts.
Figure 3.

- Far from the draconian price setting Big Pharma has complained about, AstraZeneca CEO Pascal Soriot told a Senate committee recently that initial steps in Medicare negotiation are positive: “So far, what we’ve seen is relatively encouraging.”
- Raymond James analyst Chris Meekins wrote: “As we have been saying since the Inflation Reduction Act first passed, we believe the sector-wide impact of the Inflation Reduction Act, including negotiation, on the pharmaceutical industry to be minimal.”
Taxpayers are the source of early high-risk, basic science that drives innovation — not industry.
- The National Institutes of Health (NIH) is the single largest source of biomedical research in the world. Its budget in 2023 was almost $48 billion. The NIH contributed to research associated with all 356 new drugs approved by the FDA from 2010-2019, totaling more than $230 billion.
- The reason President Biden has established the Cancer Moonshot and the Advanced Research Projects Agency for Health (ARPA-H) with billions in funding to accelerate early, high-risk research is because Big Pharma won’t take the risks on its own. Taxpayers must underwrite this early work to find bold new treatments and perhaps cures.
Lower drug prices help people access existing, innovative drugs they need right now, but can’t afford.
- Innovation is worthless if people can’t access it.
- CBO reports one of the ways the IRA saves money is by improving adherence to drug therapies which leads to better health because lower prices enable more people to buy and use their drugs as directed.
Finally, Big Pharma consistently threatens that patients will lose access to newly developed drugs. It notes that more drugs are available — and are available faster — in the United States than in other wealthy countries. Pharma frequently cites a white paper from the White House Council of Economic Advisers (CEA) to explain why: “Drug manufacturers usually pursue market access in the United States before other markets due to the higher prices in the United States.” The CEA could also have mentioned the other big reason drug companies file for approval first in the United States: It is the largest market in the world., After the IRA is fully implemented our country will still offer the highest prices by far in the largest market in the world, preserving the incentive to file first for approval in the United States.
There are other important policies in the U.S. drug pricing system that lead to more drugs being available here compared to other countries, none of which are altered by lowering prices under the IRA:
- Medicare must cover all drugs in six protected classes, which even the Pharmaceutical Research and Manufacturers of America (PhRMA) acknowledges ensures access to these drugs.,
- Medicare must cover at least two drugs in each class of drugs.
Medicaid must cover every drug offered by a manufacturer in the United States if the manufacturer agrees to give Medicaid a best-price guarantee.
The pharmaceutical industry’s threats to innovation and access don’t hold up. The IRA restores balance to move us in the direction of fair prices and profits while still getting the innovation we need.
Section VI: Conclusion
Let’s be clear: Big Pharma is not fighting for the interest of patients or because lowering its prices a bit will cripple innovation. It’s fighting to restore and maintain its complete economic power over the American people to dictate prices of brand-name drugs–a power it has in no other nation on the planet. The head of the powerful trade association, PhRMA, affirmed that fact in a moment of candor when he said in an interview a couple of years ago that his industry is “particularly adept at … rolling the tanks, if you will, to push back against policy proposals adverse to the industry’s interests.” The industry’s multiple lawsuits to block Medicare negotiation that will touch only about four percent of its global revenue is further evidence this struggle is about keeping the U.S. market as the one place in the world where it can dictate prices at the expense of people’s lives and livelihoods.
Of course, drug companies want to disguise that truth. Instead, they blame others and never offer policy solutions that involve lowering their prices. They seek to distract attention from their central role in making drugs unaffordable in America today.
And they try to scare us by saying that if we don’t bend to their will, we won’t get the drugs we need for the future. They pose questions like: How much would you pay to save a life?
And that’s easy. When it’s you or someone you love, the answer is anything. You’ll empty your bank account, mortgage your home, cash out your 401k. You’ll do whatever you have to do.
But that’s the wrong question. We should be asking: How do we strike and maintain a balance to ensure we get the innovation we need at prices we can afford?
While we at Patients For Affordable Drugs NOW would have gone further in the Inflation Reduction Act, it clearly was built with the goal of striking that balance as a foundational principle. That point is driven home by a fact that is worthy of repeating: The IRA does not change the key way our nation rewards investment and risk-taking for innovation–we continue to allow drug companies to set launch prices and maintain those prices for a minimum of nine to 13 years before potentially facing negotiated prices.
This story from John in Baltimore captures so well the challenges patients face and the need to lower drug prices. Like me, he has multiple myeloma and must take very expensive drugs. He says: “I’m on a tightrope that is scarier than the disease itself. I did everything to protect myself and my family from financial disaster, but I feel as though after everything I’ve been hijacked by a drug company. I have no other options and they want to keep it that way.”
I feel incredibly grateful to spend my retirement fighting so John can feel secure in his retirement, and not be held hostage by a drug company. I ask that you help John and millions of other Americans by moving forward with bipartisan patent and PBM reforms to make our system work better for the people it is supposed to serve.
Thank you.