Click here for a downloadable PDF
Statement of David E. Mitchell Founder, Patients For Affordable Drugs Now to the Subcommittee on Health of the United States House Of Representatives Energy and Commerce Committee for a hearing on “Legislative Proposals to Support Patients with Rare Diseases”
February 29, 2024
Section I. Background and Introduction
I want to thank you for holding this hearing “to discuss solutions to support patients living with rare diseases.” I am one of those patients. My name is David Mitchell. I am the founder of Patients For Affordable Drugs Now. We are the only national patient advocacy organization focused exclusively on policies to lower prescription drug prices. We are independent, bipartisan and we don’t accept funding from any organizations that profit from the development or distribution of prescription drugs.
Since we launched seven years ago, we have collected over 34,000 stories from patients across all 50 states struggling to pay high drug prices. And we have built a community of over three-quarters of a million patients and allies supporting policies to lower drug prices.
More importantly for today, I am a rare disease patient. I have a rare, incurable blood cancer, and prescription drugs are keeping me alive — literally.
My oncologists currently have me on a four-drug combination of infused and oral cancer drugs. These four drugs carry a combined list price of more than $1 million per year. Just one of my oral drugs, called Pomalyst, is priced at more than $22,400 for 21 capsules, which I must buy every 28 days. And because Medicare beneficiaries like me pay our out-of-pocket costs based on list price, I spent more than $16,500 out-of-pocket last year — just for Pomalyst. To help manage the cost of my infused drugs, I spend another $3,731 per year to purchase a Part B supplement. And of course, I have the base costs of Medicare to pay as well.
For people with my cancer — multiple myeloma — drugs account for 60 percent of the cost of treatment. Sixty percent.
I am a very lucky man — these drugs are currently keeping my cancer at bay, and I tolerate them pretty well. But the reason I am on four drugs is because each began to stop working, so the doctors first increased the dose, then increased the frequency, and then added another drug. Eventually, I will fail on this combination, too. When that happens, I will be what is called “triple refractory” to all of the three major classes of drugs used to treat my disease. The cancer will begin to increase in my blood and I will need a new treatment. Fortunately, there are options out there.
But one of the new drugs approved recently that I might be a candidate for carries a list price of $465,000. That’s just for the drug — it doesn’t cover the hundreds of thousands of dollars required to administer the drug and manage my health in the wake of the treatment. And each of the new drugs comes with its own risks: The treatment I am referring to is called Chimeric Antigen Receptor T-Cell therapy (CAR-T) and it carries a black box warning that it may actually cause secondary cancers. I don’t know what’s ahead in my journey as a cancer patient.
But the point is: I need these innovative new drugs. I care deeply about innovation and new drug development. My life depends on it. Without innovation, I will die sooner than I hope to. That is just an unfortunate fact.
But my more than 13-year journey as a cancer patient has taught me one irrefutable fact: Drugs don’t work if people can’t afford them.
Section II. The Price of Drugs and Need for Further Reforms
Drugs are too expensive in the United States, and there is no justification for the high prices. When drug makers hike prices each year, they don’t do so because the drug becomes more valuable. Drug companies raise prices because they can. We let them.
The result is that Americans pay more than four times what people in other wealthy nations pay for the exact same brand-name drugs. Even after applying an estimate of rebates to arrive at net prices, Americans are paying more than three times what people in other wealthy nations pay for the same brand name drugs.
Consequently, about three in ten Americans report having difficulty affording their medications. When their prescription drug prices are too high, Americans face challenges affording other expenses, such as food and housing. One survey found that over 20 percent of people took on debt or declared bankruptcy because of their medications.
High drug prices disproportionately harm communities of color. One in two Latinos in the United States takes a prescription medication, and more than 20 percent are uninsured. Black and Latino adults aged 65 and older were more likely to report difficulty affording prescription medications than White adults. Further, Black Americans are more likely to live with chronic pain, diabetes, and high blood pressure than white Americans and are nearly two times more likely to be uninsured.
As expensive as my drugs are, even with Medicare, I never lose sight of the fact that roughly 26 million Americans don’t have any health insurance at all and are exposed to the full list price.
People struggle to pay the prices with and without insurance.
Americans have been demanding relief for years. A KFF poll in July of 2023 found three out of four Americans said there is not enough government regulation when it comes to limiting the price of prescription drugs. That includes 82 percent of Democrats, 67 percent of Independents, and 68 percent of Republicans. In the wake of the enactment of the Inflation Reduction Act which is helping millions of people–Americans want more done.
Section III. The Inflation Reduction Act Is A Huge Step Forward Helping Millions Of People
The historic Inflation Reduction Act (IRA) is lowering prescription drug prices and reducing out-of-pocket costs for millions of people in this country. The benefits include:
- Insulin costs in Medicare are capped at $35 monthly. “About 1.5 million Medicare beneficiaries who use insulin would have saved $734 million in Part D and $27 million in Part B out-of-pocket costs in 2020 if these caps had been in effect in 2020.”
- Recommended vaccines that would have cost $100-200 per vaccination are now free under Medicare Part D. “In 2021, 3.4 million people received vaccines under Part D, and annual out-of-pocket costs were $234 million.”
- Due to the inflation rebates under the IRA, “Medicare Part B beneficiaries have already enjoyed lower coinsurance for 20 drugs from April 1 to June 30 and for 43 drugs from July 1 to September 30 2023”
- Low-income subsidies were expanded starting January of this year. The “expanded financial assistance in Medicare’s Low-Income Subsidy (LIS) Program would have benefited nearly 461,000 Partial LIS enrollees had the provision been in effect in 2020. An additional 2.9 million Part D enrollees who were eligible but not enrolled in LIS would also have benefited from the program.”
- Starting in 2026, negotiated prices will take effect on 10 of the highest-cost drugs for Medicare, lowering prices and out-of-pocket costs for millions of beneficiaries. That number will rise to 60 drugs in the coming years, extending the benefits of negotiation to many more millions of people.
“The Inflation Reduction Act’s redesign of Medicare Part D, including a $2,000 out-of-pocket cap is estimated to reduce enrollee out-of-pocket spending by about $7.4 billion annually among more than 18.7 million enrollees (36 percent of Part D enrollees) in 2025 – nearly $400 per person among enrollees who have savings in out-of-pocket costs under the IRA.” The IRA annual Medicare out-of-pocket spending limits began to phase in this year, and people taking expensive brand-name drugs will see their spending capped at the catastrophic level at about $3,300-3,500.
Let me tell you about my personal experience with the phasing in of the out-of-pocket cap this year. My total out-of-pocket expense for all my Medicare Part D drugs last year was $16,916 because there was no out-of-pocket cap in place. This year, thanks to the IRA’s phasing in of an out-of-pocket cap for beneficiaries who reach the catastrophic phase of the benefit this year, I paid $3,308 for my first fill of Pomalyst and will be paying no more out-of-pocket for Pomalyst or any of my Part D drugs for the rest of the year. That’s a savings of more than $13,600. For so many patients who are stuck with diseases or chronic conditions that require high-priced brand drugs, it is life-changing.
Take Sue from Wilmington, Delaware. She writes: “I have Waldenstroms Macrobulemia, a form of blood cancer. I take Imbruvica which is $18,000 a month. After insurance, I pay the first $8,000 in 2-months copay and then $1,000 a month thereafter. I am 76 years old and working full time to afford this medication.” Sue will save between $12,000-14,000 this year with the out-of-pocket cap phasing in.
It’s critical to remember that the way out-of-pocket costs are being reduced without unacceptable premiums or tax increases is by lowering the underlying prices of drugs in Medicare. If Congress weakens the IRA allowing higher prices than the law as written will deliver, we will see higher costs to both beneficiaries like Sue and myself, the government, and taxpayers.
Section IV. The Inflation Reduction Act Achieves Balance To Ensure Innovation We Need At Prices We Can Better Afford
In the run-up to the enactment of the IRA, the drug industry kept telling us that the legislation would stifle investment and kill innovation and access to new drugs. No one cares more about innovation than patients. But if you pull back the curtain on this pharma fear-mongering and look at what has actually happened since the IRA enactment, the argument doesn’t hold up. Here are nine reasons why.
The industry has plenty of money for innovation. In the wake of the Inflation Reduction Act passage, investors are upbeat. Drug company stocks are doing fine. The industry is flush with cash and has great access to capital.
According to the Congressional Budget Office (CBO), despite Big Pharma’s claims that the implementation of the Inflation Reduction Act would stifle innovation and significantly impact profit margins, there has been a consistent and continuous increase in venture capital investment in pharmaceutical companies, demonstrating stability and resilience within this sector as shown in Figure 1.
Figure 1.
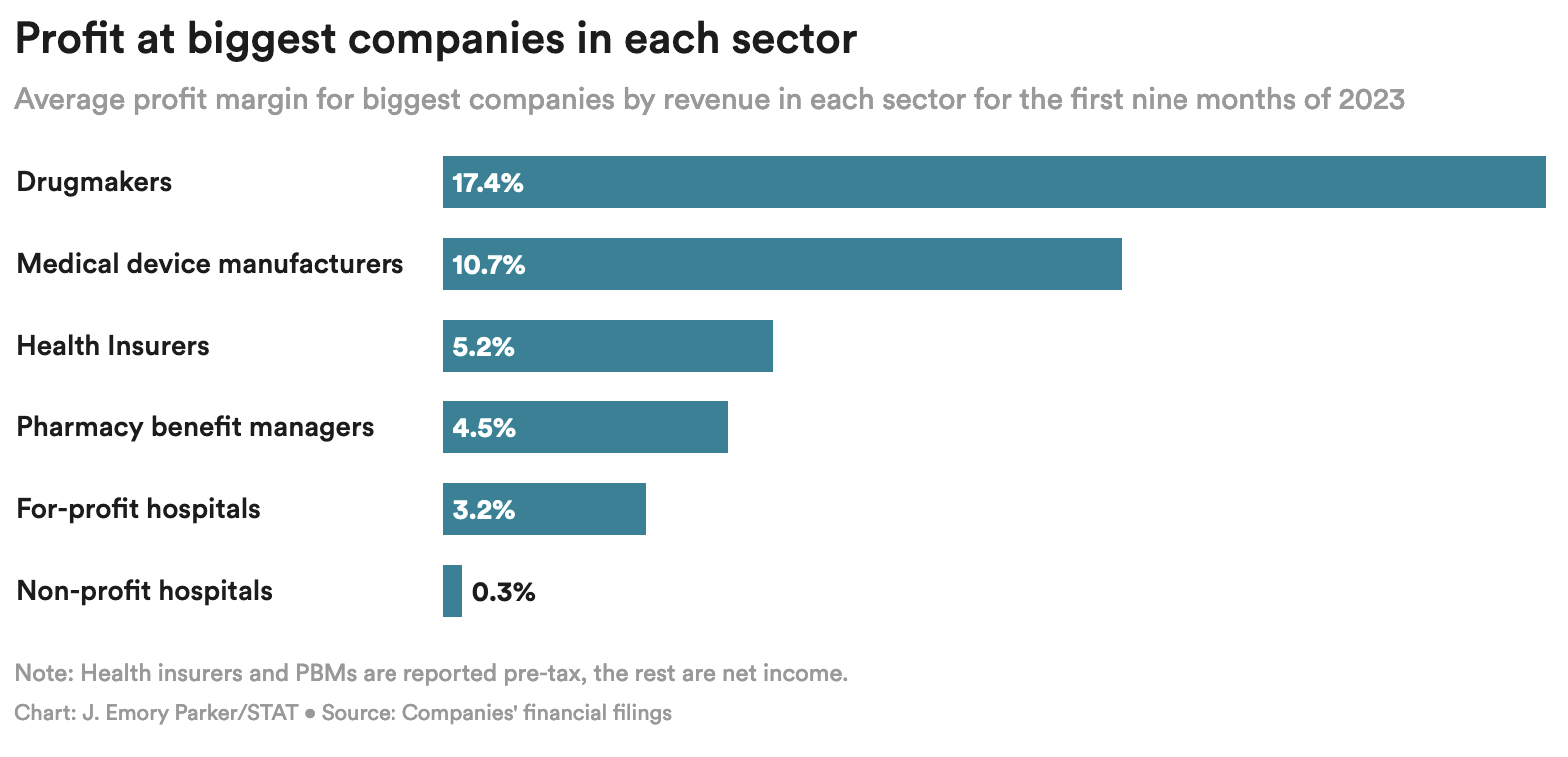
Drug companies are flush with cash and remain by far and away the most profitable sector of the healthcare industry–more than tripling the profit of Pharmacy Benefit Managers (PBMs) and insurers.
Figure 2.
Since the passage of the Inflation Reduction Act:
- Pfizer acquired biotech company Seagen for $43 billion.
- Sanofi bought a diabetes product company for $2.9 billion.
- Novartis spent $15 billion in a stock buyback.
- Even in the face of the Inflation Reduction Act, drug companies reported increased investment in research and development (R&D). For example, in 2022 10-K filings, Johnson & Johnson reported an 11.8 percent increase in R&D spending in 2022, Merck reported an 11 percent increase in R&D spending, and Moderna reported a 65 percent increase in R&D spending and projected further increases in 2023.
- “Bayer plans to invest $1 billion on research and development this year in an effort to double its sales in the United States within a decade.”
- Sanofi said that it would increase the number of Phase 3 studies it is conducting by 50 percent between 2023 and 2025 at a financial cost of about $700 million a year.
The Inflation Reduction Act incentivizes innovation by curbing drug companies’ ability to drive profits by raising prices on old drugs at will.
- To make more money, drug companies will have to develop high-value new drugs that can command high prices, instead of repurposing old products.
- The negotiation process includes the consideration of therapeutic advances and meeting unmet needs, which will reward more innovative drugs.
- The law maintains the key incentive for innovation that currently exists in the U.S. by allowing drugmakers to be compensated handsomely for investment and risk by setting their launch prices, maintaining the Food and Drug Administration (FDA)-awarded period of exclusivity, and exempting all medications from negotiated prices for a 9 to 13 year period.
- The U.S. will continue to pay the highest drug prices and offer the largest pharmaceutical market in the world. Drug companies will continue to innovate in order to have access to such a lucrative market.
The Congressional Budget Office (CBO) says the Inflation Reduction Act will have a minimal to non-existent impact on new drug development.
- According to the CBO, the Inflation Reduction Act will decrease the number of new drugs over the next 30 years by only about 15 out of 1,300 expected – that’s only a little over one percent.
- Since only 10 to 15 percent of “new” drugs represent true therapeutic advancements, of the 15 new drugs foregone, only one or two might actually be true innovations.
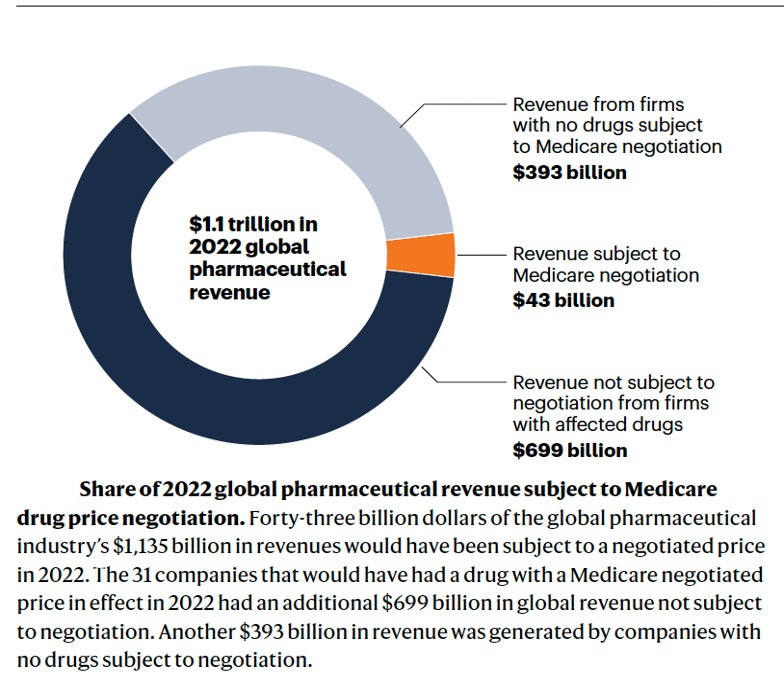
- Pharma cries poor every time policy reforms take even a small piece of change out of its pocket. But the reduction in drug industry revenue from the Inflation Reduction Act will be very small overall — estimated at less than one percent through 2032. Figure 3 shows we are barely making a dent in the drug industry’s global revenues with Medicare negotiation, which the industry is spending an enormous sum of money to prevent in the courts.
Figure 3.
- Far from the draconian price setting Big Pharma has complained about, AstraZeneca CEO Pascal Soriot told a Senate committee a few weeks ago that initial steps in Medicare negotiation are positive: “So far, what we’ve seen is relatively encouraging.”
- Raymond James analyst Chris Meekins wrote: “As we have been saying since the Inflation Reduction Act first passed, we believe the sector-wide impact of the Inflation Reduction Act, including negotiation, on the pharmaceutical industry to be minimal.”
Taxpayers are the source of early high-risk, basic science that drives innovation — not industry.
- The National Institutes of Health (NIH) is the single largest source of biomedical research in the world. Its budget in 2023 was almost $48 billion. The NIH contributed to research associated with all 356 new drugs approved by the FDA from 2010-2019, totaling more than $230 billion.
- The reason President Biden has established the Cancer Moonshot and the Advanced Research Projects Agency for Health (ARPA-H) with billions in funding to accelerate early, high-risk research is because Big Pharma won’t take the risks on its own. Taxpayers must underwrite this early work to find bold new treatments and perhaps cures.
Lower drug prices help people access existing, innovative drugs they need right now, but can’t afford.
- Innovation is worthless if people can’t get access to it.
- CBO reports one of the ways the IRA saves money is by improving adherence to drug therapies which lead to better health through lower prices.
The American public no longer buys Big Pharma’s threats to innovation. Policymakers shouldn’t fall for them either.
- Bipartisan polling shows that American voters do not buy drug industry arguments against drug price reform, as nearly 80 percent of respondents say the pharmaceutical industry can live with slightly lower profits and still provide the innovation patients need.
Finally, Big Pharma consistently threatens that patients will lose access to newly developed drugs. It notes that more drugs are available — and are available faster — in the United States than in other wealthy countries. Pharma frequently cites a white paper from the White House Council of Economic Advisers (CEA) to explain why: “Drug manufacturers usually pursue market access in the United States before other markets due to the higher prices in the United States.” The CEA could also have mentioned the other big reason drug companies file for approval first in the United States: It is the largest market in the world., After the IRA is fully implemented our country will still offer the highest prices by far in the largest market in the world, preserving the incentive to file first for approval in the United States,
There are other important policies in the U.S. drug pricing system that lead to more drugs being available here compared to other countries, none of which are altered by lowering prices under the IRA:
- Medicare must cover all drugs in six protected classes, which even the Pharmaceutical Research and Manufacturers of America (PhRMA) acknowledges ensures access to these drugs.,
- Medicare must cover at least two drugs in each class of drugs.
Medicaid must cover every drug offered by a manufacturer in the United States if the manufacturer agrees to give Medicaid a best-price guarantee.
The pharmaceutical industry’s threats to innovation and access don’t hold up. The IRA restores balance to move us in the direction of fair prices and profits while still getting the innovation we need.
Section V. H.R. 5547 and H.R. 5539 Are Misguided Because They Are Based On False Premises
H.R. 5547 is a solution in search of a problem that doesn’t exist in actuality and is only being raised by the industry to reduce the impact of Medicare negotiation and keep prices on more drugs higher for longer. The supposed problem posited by industry is that relative to the previous law, the reforms in the Inflation Reduction Act economically disadvantage small-molecule drugs compared to biologics, which will hurt innovation, increase prices, and harm the people who need these medicines.
This claim is completely misleading, and unsupported by the facts. The Inflation Reduction Act actually narrows the advantage for biologics over small molecules.
The pharma industry’s complaint is specious, which can be seen clearly in that, over time, its stances have been completely inconsistent. Biologics were given a huge advantage over small-molecule medicines because the pharmaceutical industry insisted on receiving seven years more market exclusivity for biologics than for small-molecule drugs when the Biologics Price Competition and Innovation Act (which was included in the Affordable Care Act) was being structured., , ,
Here’s what the trade association BIO said to justify a longer period of exclusivity for biologic drugs:
“Biologics research and development is a high-risk endeavor, with higher capital costs, higher material costs, greater manufacturing costs and uncertainties, longer development times, and lower late-stage success rates than compared to small molecule drugs.”
At the time, the pharmaceutical industry did not suggest that this enormous advantage for biologics would lead to the development of fewer small-molecule drugs, which it didn’t. Since 2010, more than 75 percent of new drugs approved by the FDA have been small molecules.
The Inflation Reduction Act actually contains more generous incentives for small-molecule medicines because it narrows the difference in years of exclusion from Medicare negotiation between biologics and small molecules to four years. And the negotiation exemption periods for small molecules (nine years) and biologics (13 years) are longer than the existing market exclusivity periods granted by the Food and Drug Administration (FDA), which are five years and 12 years, respectively.
Drug companies now assert that both types of drugs should be treated equally for purposes of negotiation — pharma’s chosen solution is, naturally, to increase the exemption period for small molecules to 13 years to match that of biologics. To put this into perspective, other high-income countries provide small-molecule and biologic drugs with identical periods of market exclusivity. The only reason the U.S. is not on that list is because the pharma industry lobbied the United States Congress aggressively for a longer monopoly period for biologics.
This misleading complaint — that the Inflation Reduction Act will stifle the development of small molecule drugs — is not supported by facts and is inconsistent relative to the pharmaceutical industry’s long-held positions on the need for advantageous treatment for biologic drugs.
In fact, since the enactment of the IRA, investment in small molecules has not declined–it has increased and investors are bullish:
- In the 9 months following the passage of the IRA, big drug companies acquired more small-molecule drugs than in the 9 months preceding the law, indicating drug companies still find small molecules an attractive investment.
- Industry sources are projecting nearly 8 percent annual growth in small molecule sales for the years 2022 to 2032 which amounts to a doubling of sales over the period.
- Bristol Myers Squibb has signed a $4.8 billion deal to buy Mirati Therapeutics and its small molecule cancer drug Krazati.
- Lilly spent $2.4 billion to acquire a small molecule drug for development in July 2023.
- Forward Therapeutics secured $50 million in Series A financing, signaling robust investor confidence in advancing next-generation small molecule therapies for chronic immunological and inflammatory disorders.
- Respected venture capitalist, Vineeta Agarwala of Andreessen Horowitz, said recently: “Every Pharma company, despite the IRA, is talking about small molecules.”
- Another of biotech’s biggest financiers, venture capital company Flagship Pioneering, says: “Flagship continues to see great value in developing small molecule drugs. The IRA hasn’t changed that.
The so-called “pill penalty” seems simple on its face, which no doubt is part of the reason pharma picked it as a rallying cry. But, if you do the math, it’s easy to see just how ridiculous the industry argument is. Drug companies will still continue to make massive profits on small molecules. To qualify for negotiation, a drug must, among other things, have annual Medicare sales of at least $200 million. Given that Medicare accounts for roughly 30 percent of total U.S. sales, an eligible drug would have more than $600 million in annual U.S. sales. Nine years of sales at $600 million annually produces revenue of more than $5.4 billion. Based on independent research, it costs an average of less than a billion dollars to bring a new drug to market–including covering costs of failures. That means a company with a drug qualifying for negotiation can easily make more than a 500 percent return on a small molecule before facing negotiated prices in Medicare. In fact, this simple math exercise greatly underestimates how much revenue these small molecule drugs can command when you consider that in 2023 average sales of small molecule drugs protected by exclusivity with over $200 million in annual revenue and nine or more years on the market is actually $2.86 billion.
The simple fact is that healthy profit is guaranteed on safe and effective small-molecule drugs because the IRA allows drug companies to set initial launch prices. That is the principal way we reward risk and investment to bring an innovative drug to market, and nothing in the IRA changed that core element of our system. Companies can set prices to ensure a healthy return before possibly being selected for negotiation. It is a no-lose proposition.
All of these points apply to the gene technologies that are the focus of H.R. 5547. With 5,000 gene therapy trials listed at the NIH–if only 10 percent come to market, mandating 13 years of exclusivity instead of nine years before negotiated prices take effect would raise Medicare spending dramatically.
The whole argument about 9 vs 13 years is not really about the interests of the millions of Americans who rely on medicines to get healthy — or stay alive. The drug industry simply wants 13 years of exemption from negotiated prices for all drugs to make as much profit as possible. Period. If drug companies now want equal timing for the negotiation of all drugs, we should equalize them all at nine years.
H. R. 5539 proposes to undo a critical reform in the IRA to ensure drug companies can’t abuse orphan drug status.
This issue deeply affects patients including myself. I have an orphan disease and three of the four cancer drugs I am currently taking were initially approved as orphan drugs–Velcade, Darzalex, and Pomalyst., , We need to protect incentives for orphan drug development, but we must stop the abuse of the orphan drug designation which extends monopolies indefinitely and hurts patients through the imposition of unjustified high prices.
The abuse of orphan status by drug companies was documented in detail by Kaiser Health News (KHN now KFF News) more than seven years ago. Here is a key conclusion from that investigation:
“‘What we are seeing is a system that was created with good intent being hijacked,’ said Bernard Munos, a former corporate strategy advisor at drug giant Eli Lilly and Co. who reviewed the KHN analysis of several FDA drug databases. It’s ‘quite remarkable that it has gone on for so long.’”
It’s time for the abuse to stop while protecting key incentives for orphan drug development, and that is exactly what the Inflation Reduction Act does.
- Orphan drugs that treat a rare disease with a patient population of less than 200,000 are excluded from negotiation completely.
- Small biotech firms – many of which make orphan drugs – are excluded from negotiation until 2028.
- All existing incentives for orphan drug development are maintained, including tax credits for clinical trials and granting of priority review vouchers, worth more than $100 million.
- Orphan drugs with more than one indication for small patient populations – or even multiple indications – are highly unlikely to ever be included in negotiation because they won’t ever meet the spending threshold.
- It will be almost impossible for drugs with multiple ultra-rare designations to ever reach spending levels to qualify for negotiation.
- About 50 percent of rare diseases are pediatric, and children, with very few exceptions, do not qualify for Medicare. Their treatment is paid for by other payers, such as Medicaid and commercial health plans, which don’t have access to the payment rates that Medicare ends up negotiating. So negotiation will have little to no impact on pediatric drug development.
- Drug companies can still make increased revenue by expanding the populations they treat with additional orphan designations before negotiation should they qualify for negotiation, and turn a pretty profit in Medicare even after negotiation. It may just not be as big a profit as they would like.
Consistent with the overall approach of the IRA, the orphan drug provisions strike a balance that will stop abuse of patients by drug companies while still maintaining strong incentives for continued orphan drug development.
Section VI. What Else Should We Do? Curb Patent Abuse and Reform Pharmacy Benefit Managers (PBMs)
Patents For Innovation–Not To Block Competition and Lower Prices
When a drug company makes a truly innovative discovery, it should be rewarded with a patent and receive a fair return for risk and investment. Our patent system is designed to facilitate these rewards for innovation so that drug companies are incentivized to pursue true clinical breakthroughs and inventions that bring meaningful benefits to patients.
But the drug industry would have you believe that every patent is deserved and that the sheer volume of patents granted is an appropriate indicator of innovative achievements. That couldn’t be further from the truth.
Neither new patents nor new drugs equal new innovation. Worse, manufacturers are abusing America’s patent and exclusivity system in too many cases to prevent free-market competition and block affordable generic and biosimilar drugs from coming to market.
Between 2005 and 2015, at least 78 percent of the new drug patents issued were for drugs already on the market.
Of the roughly 100 best-selling drugs, nearly 80 percent obtained additional patents to extend their monopoly period.
In fact, gaming of the patent system to extend monopolies beyond the time intended under law inhibits true innovation that patients like me and millions of others need. If drug companies can block competition and raise prices at will on old drugs to drive profits and executive bonuses, they have far less incentive to take risks and invest in Research and Development (R&D) to find innovative new drugs that could command high prices and save lives.
There are a variety of strategies used by drug corporations to extend monopolies, including product hopping, patent thicketing, pay-for-delay deals, and abuse of the Food and Drug Administration’s (FDA) citizen petition process. All of these practices thwart competition and allow drug corporations to keep drug prices high. There have been several bipartisan pieces of legislation advanced in this Congress to address these issues and allow for more generic drugs and biosimilars to enter the market, which is critical to making drugs more affordable for patients.
P4ADNow strongly supports H.R. 3839, which was included in the Lower Costs, More Transparency Act, and passed the House on a strong bipartisan vote. In addition, P4ADNow supports bipartisan legislation that would reduce patent thicketing, curb product hopping, ban pay-for-delay agreements, reduce abuse of citizen petitions at the FDA, and improve coordination between FDA and the US Patent Trademark and Office (USPTO). Importantly, all of these measures would produce billions of dollars in savings that could be used to offset other health care priorities.
We must ensure patents are used as intended to reward true invention and innovation–not to extend monopolies and block lower prices through competition. To achieve true innovation at prices we can afford over the long haul, we must reform our patent and exclusivity system.
Increase Transparency and Stop Anticompetitive Practices By Pharmacy Benefit Managers (PBMs)
While the headwaters of our drug pricing problems are the list prices set by drug corporations, there are other reforms needed downstream in the supply chain. Pharmacy benefit managers (PBMs) are black boxes that cut secret, mutually beneficial rebate deals with manufacturers, and none of it is transparent.
It is simply wrong that patients like me don’t know if the preferred drug on a PBM formulary is there because it is the best drug, because it is the least expensive drug among equally effective options, or because the PBM got a big, legal kickback from the manufacturer. Without transparency, it is impossible to know how much of a rebate is going to the PBM, to the insurer, to lower my premiums, or to reduce my out-of-pocket costs at the pharmacy counter. With the Big Three PBMs–Cigna, Optum Rx, and CVS Health–in control of 80 percent of the $633 billion in U.S. spending on drugs, that is more than half a trillion dollars flowing through just those three entities annually., And vertical integration uniting all three major PBMs with insurers only increases their market power. Opaque practices with that kind of money involved are a bad way to run a railroad. It’s time for transparency to ensure PBMs are operating in the best interests of those they are supposed to serve — patients and consumers.
Drug companies and PBMs also enter into rebate arrangements that are designed to thwart lower-cost competition. These are commonly called “rebate walls,” defined as:
“Exclusionary contracting practices that a drug manufacturer deploys to limit the ability of rivals from gaining preferred access to the formulary, or any access at all. Branded manufacturers leverage their position as market leaders by offering financial incentives to pharmacy benefit managers and health insurers in the form of ‘all or nothing’ conditional volume-based rebates, in exchange for virtually exclusive positioning on the formulary. …If the payer does not accept the rebate agreement for a particular indication, it may lose all rebates for its product on all covered indications.”
Let’s be clear: These deals are designed to benefit both the manufacturer seeking to block competition and the PBM that gets a bigger rebate. These deals are not designed to help patients like me by lowering prices or increasing patient choice. They are emblematic of our drug pricing system which has been built to benefit those who profit from it at the expense of those it is supposed to serve.
P4ADNow supports reforming the practices of PBMs, including transparency requirements in order to determine how rebates are actually working — how much is going to reduce premiums and out-of-pocket for patients and consumers and how much is going to increase profits for the PBMs or insurer plan manager.
We’re pleased that the Lower Costs, More Transparency Act included several provisions to improve PBM transparency and eliminate spread pricing, among other elements. We also support reforms to “de-link” administrative fees from drug prices and to pass more of the savings collected through negotiated discounts along to patients and consumers whether through lower prices, lower out-of-pocket, or lower premiums. We hope that Congress will consider many of these measures for inclusion in upcoming health care legislation.
We are also following closely and supporting the Federal Trade Commission (FTC) investigation of these issues as well. We hope Congress will ensure the ability of the FTC to seek damages and monetary penalties for consumer protection and competition cases.
Section VII: Conclusion
Let’s be clear: Big Pharma is not fighting for the interest of patients or because lowering its prices a bit will cripple innovation. It’s fighting to maintain its economic power over the American people to dictate prices of brand-name drugs–a power it has in no other nation on the planet. The head of the powerful trade association, PhRMA, affirmed that fact in a moment of candor when he said in an interview not long ago that his industry is “particularly adept at … rolling the tanks, if you will, to push back against policy proposals adverse to the industry’s interests.” The industry’s multiple lawsuits to block Medicare negotiation that will touch only about four percent of its global revenue is further evidence this struggle is about keeping the U.S. market as the one place in the world where it can dictate prices at the expense of people’s lives and livelihoods.
Of course, Big Pharma wants to disguise that truth. Instead, it blames others and distracts attention from its central role in making drugs unaffordable.
And it tries to scare us by saying that if we don’t bend to its will, we won’t get the drugs we need for the future. It poses questions like: How much would you pay to save a life?
And that’s easy. When it’s you or someone you love, the answer is anything. You’ll empty your bank account, mortgage your home, cash out your 401k. You’ll do whatever you have to do.
But that’s the wrong question. We should be asking: How do we strike and maintain a balance to ensure we get the innovation we need at prices we can afford?
While Patients For Affordable Drugs Now would have gone further in the Inflation Reduction Act, it clearly was built with striking that balance as a foundational principle. That point is driven home by a fact that is worthy of repeating: The IRA does not change the key way our nation rewards investment and risk-taking for innovation–we continue to allow drug companies to set launch prices and maintain those prices for a minimum of 9 to 13 years before potentially facing negotiated prices.
This story from Cheryl in Louisville captures so well the challenges patients face and the need to lower drug prices. Cheryl writes: “All my inhalers, like Trelegy, are such a high cost, I do without until I have a bad episode. These inhalers cost from $350 to $800 a month. This is crazy just to be able to breathe every day. Something is wrong here.”
Cheryl is right. I feel incredibly grateful to spend my retirement fighting to fix what’s wrong so that people like Cheryl can one day enjoy theirs. We must protect the Inflation Reduction Act from being weakened. And we must move ahead with patent and PBM reforms to make our system work better for the people it is supposed to serve with lower prescription drug prices for all.
Thank you.