Vice President Joe Biden Pledges to Lower Drug Prices
NASHVILLE, Tenn. — During tonight’s presidential debate in Nashville, Vice President Joe Biden promised to stand with patients and let Medicare negotiate for lower drug prices.
“Drug prices are a top issue for voters, and we appreciate Vice President Biden emphasizing his plan to lower prices, promote competition, and let Medicare negotiate,” said Ben Wakana, executive director of Patients For Affordable Drugs Now.
Vice President Biden: “We’re going to make sure we reduce the premiums and reduce drug prices by making sure that there’s competition that doesn’t exist now by allowing Medicare to negotiate.”
BACKGROUND:
Nearly 9 out of 10 voters say lowering prescription drug prices is a top health care issue deciding their 2020 presidential vote.
86 percent of Americans support “allowing the federal government to negotiate with drug companies to get a lower price on medications for people on Medicare.”
According to the University of Pennsylvania, Vice President Biden’s proposals would lower average prescription drug prices by roughly 60 percent.
Vice President Joe Biden’s plan to lower drug prices has several key components:
Allow Medicare to negotiate for lower prices and limit price increases for brand-name drugs to the rate of inflation
Create policies to counter anti-competitive practices like “pay-for-delay” deals, patent thickets, and evergreening
Evaluate the role of taxpayer investments in R&D and factor it into pricing decisions
Drug prices are continuing to rise, with increases on over 500 drugs in January 2020 alone and nearly 250 additional drugs in the first six months of the COVID-19 pandemic.
###
WASHINGTON, D.C. — Patients across the country are calling on President Trump and former Vice President Biden to discuss their plans to lower the prices of prescription drugs at the final presidential debate in Nashville Thursday.
“Ever increasing drug prices continue to hurt Americans all across the country,” said David Mitchell, a cancer patient and the founder of Patients For Affordable Drugs Now. “And with the pandemic stealing lives and livelihoods, voters need to hear from the candidates about how they will lower the prices of prescription drugs. We will be listening as the candidates lay out their final arguments Thursday — to hear how they will fight for patients and stand up against pharma.”
According to the Kaiser Family Foundation, nearly 9 out of 10 voters say lowering prescription drug prices is a top health care issue deciding their 2020 vote. And, 35 percent of voters say drug pricing is among their “most important” voting issues, according to Gallup.
Patients in 15 key battleground states have shared stories of the impact skyrocketing drug prices have had on their lives. Here’s a sample of what patients across the country want the presidential candidates to understand:
Blythe Kauhn, Chandler, AZ, type 1 diabetes: “I feel like more people need to understand that it’s not cheap to have conditions that don’t go away. We don’t get to say, ‘Oh, I don’t want to have diabetes this month.’”
Kris Garcia, Denver, CO, bleeding disorders: “When you cast your ballot, make sure your candidate has a plan to lower drug prices.”
Clayton “DJ” Martin, Jacksonville, FL, sickle cell disease: “As a father with sickle cell, with a daughter with the sickle cell trait, I worry about her future because of the high prices of drugs.”
Patricia McKenzie, Lithonia, GA, type 2 diabetes: “People have to choose between eating and their medications. They have to choose between life and death. And that should not be a choice. Not here in America.”
Jacquie Persson, Waterloo, IA, Crohn’s disease: “I’m voting for candidates who will stand up to Big Pharma and lower the prices of prescription drugs.”
Tammy de la Cruz, North Las Vegas, NV, chronic inflammatory demyelinating polyneuropathy: “The cost of this medication is anywhere from $1,000 to $1,500, and I get it every week. Without it, I fear I will become paralyzed again.”
Rose Keller, Concord, NH, cystic fibrosis: “The high cost of drug prices has stripped me, and other young patients like me, of the opportunity to dream about what we might be when we grow up.”
Don Kreis, Concord, NH, Rose’s father: “For my sake, and for the sake of my daughter, I hope you will vote for candidates who fight Big Pharma and stand up for lower drug prices.”
Steven Hadfield, Charlotte, NC, blood cancer: “The doctor has recommended me to work less. But I live in fear over my high drug prices.”
Sophie, 19, Grand Rapids, MI, type 1 diabetes: “It’s going to be my first time voting this year. Prices of drugs have a huge effect on my vote.”
Hazel, 12, Grand Rapids, MI, type 1 diabetes: “I hope you’ll vote for candidates who will fight for lower drug prices.”
Travis Paulson, Eveleth, MN, type 1 diabetes: “Since the pandemic has started, we’ve been forced to buy our medications and insulin at the extraordinary prices they charge here in the U.S.”
Heidi Kendall, Missoula, MT, chronic myeloid leukemia: “It’s scary to depend for my life on a drug that costs so much.”
Kolton Chapman, Pickerington, OH, ulcerative colitis: “When I was on Entyvio, I was responsible for paying $2,000 a month. It was more than I owe in student loans, so I ended up filing for bankruptcy because of my medical debt.”
Rachel Burnett, Pittsburgh, PA, Crohn’s disease: “It’s so unfair to have these illnesses, and it’s so unfair to have to pay so much just to stay alive.”
Candice Brown, Alexandria, VA, ulcerative colitis: “This drug pricing system was not meant to benefit me as a patient. It was meant to benefit Big Pharma.”
Leah Clark, Columbus, WI, Crohn’s disease: “I have big plans for my future, and I can’t afford to have the high cost of drug prices getting in the way of my accomplishments.”
In September, Patients For Affordable Drugs Now launched a national campaign lifting up the voices of patients who are calling on voters to support candidates who will stand up to Big Pharma and fight to lower prescription drug prices. The campaign features TV, radio, and digital ads alongside tools to give grassroots patient advocates the power to engage with candidates on the issue of drug prices. P4ADNow is an independent, bipartisan patient organization focused on policies to lower drug prices. It does not accept funding from any organizations that profit from the development or distribution of prescription drugs.
###
WASHINGTON, D.C. —This week, two independent investigations detailed how Big Pharma is showering state and federal officials with tens of millions of dollars in hopes of winning their votes in legislative fights next year.
STAT NEWS: “First-of-its-kind examination shows how widely pharma showers campaign cash at the state level”
HOUSTON CHRONICLE: “Prescription drug costs take center stage in Texas races for Congress”
“Pharma may have deep pockets, but patients have our voices and our votes,” said David Mitchell, a cancer patient and the founder of Patients For Affordable Drugs Now. “This election year, patients are sending a message to legislators at all levels: Stand with patients, not pharma.”
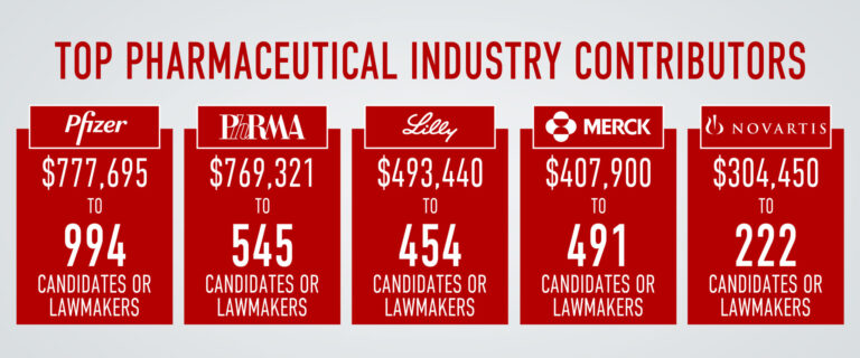
According to STAT News’ analysis, Big Pharma has conducted a coordinated effort to win favor in state legislatures. “Major pharmaceutical companies and trade groups have helped to fund the campaigns of 1,933 state legislators nationwide in the current election cycle,” according to the investigation.
The Houston Chronicle highlights the influence pharma is attempting to buy in key Texas congressional races. Nationwide, the article highlights the industry’s commitment to congressional donations: “The pharmaceutical industry had already spent $26 million on congressional campaign donations through the first six months of the year trying to influence outcomes.”
In September, Patients For Affordable Drugs Now launched an effort to push back on Big Pharma’s lobbying influence. The grassroots campaign lifts up the voices of patients and calls on voters to support candidates who will stand up to Big Pharma and fight to lower prescription drug prices.
Nearly 8 in 10 Americans say drug prices are “unreasonable,” and nearly 1 in 3 Americans report not taking their medication as prescribed due to price. According to a recent national survey, 7 out of 10 likely voters say a candidate’s position on lowering prescription drug prices is important in deciding who to vote for — including 30 percent who say it is very important.
###
WASHINGTON, D.C. —An insidious culture of greed is pervasive across the pharmaceutical industry, and today the scale of the problem was revealed. The House Oversight Committee’s investigation into drug corporations exposed a disturbing pattern of abusive pricing practices, anti-competitive behavior, and manipulative marketing campaigns.
Not a single price increase was linked to investment in research and development, according to the documents. Instead, drug corporations took unrelenting price increases to meet revenue goals, increase executive bonuses, and maximize corporate profits.
The reports examine Amgen, Novartis, and Mallinckrodt and reveal the falsehoods behind pharma’s favorite talking points.
Read highlights from the damning documents below.
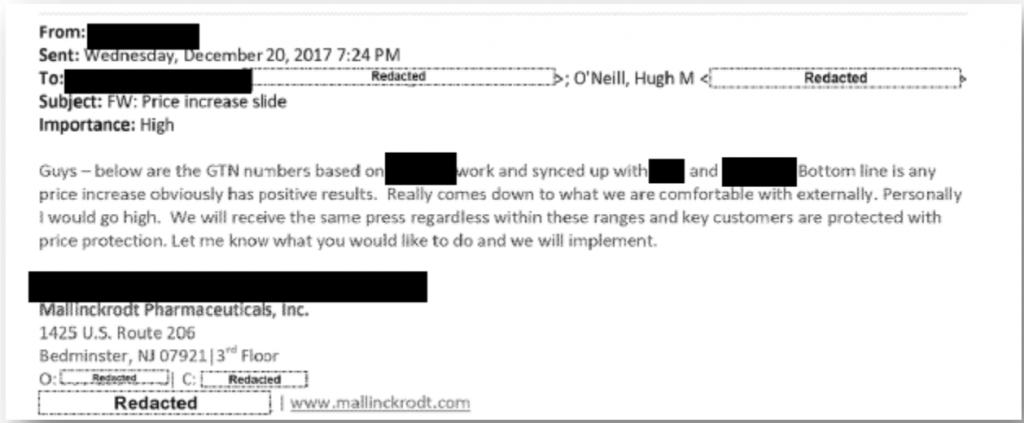
1. Pharma Claim: High prices exist to recoup R&D, not drive profits.
The reality: Executives’ motivations for price hikes is devoid of desire to recoup or invest in R&D — instead the hikes are intended to increase revenue. Internal company documents showed that company executives weighed price increases against public backlash, not the actual impact on research and development funds. Ultimately, executives decided in favor of price hikes because “we will receive the same press regardless” and “any price increase obviously has positive results.”
2. Pharma Claim: We make life-saving drugs — it’s not about the money for us.
The reality: The committee’s investigation found that executive compensation policies incentivized price hikes. Novartis increased the price of Gleevec 22 times, and its revenue soared. As a result, more than 100 Novartis employees made $1 million in 2014 and 2015.
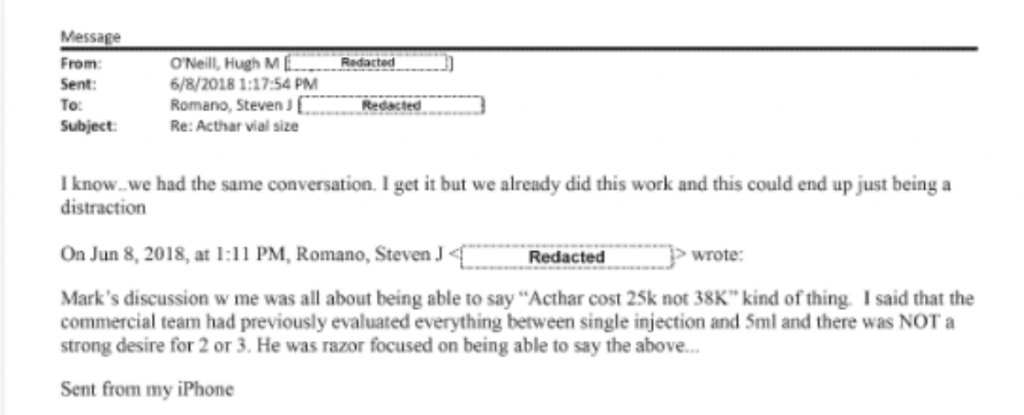
3. Pharma Claim: Our decision-making centers on the health and well-being of patients.
The reality:After public outrage at its $40,000 price for a single vial of Acthar Gel, Mallinckrodt’s CEO urged changing the vial size of Acthar gel (nearly cutting it in half) to appear like the company decreased the price.
4. Pharma Claim: Charity programs ensure our drugs are affordable and accessible.
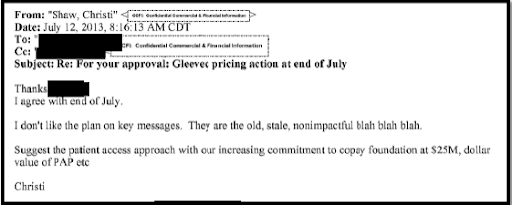
The reality:Patient assistance programs serve both as a public relations tool for companies and to increase their bottom line. Novartis’ internal strategy documents estimated the rate of return of its co-pay assistance program would be $8.90 for every dollar invested. When weighing “key messages” to employ after a highly scrutinized price hike, one Novartis executive urged colleagues to emphasize contributions to the copay foundation.
5. Pharma Claim: It’s a robust marketplace and drug companies compete based on price.
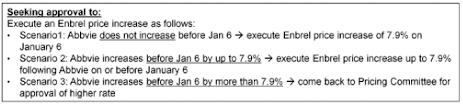
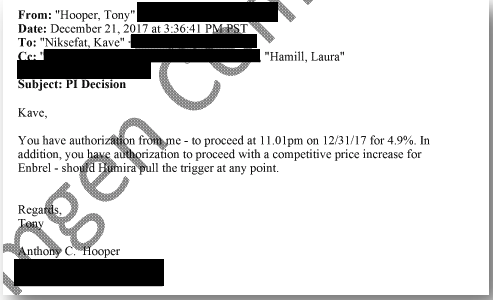
The reality: Drug companies often collude — not compete. Amgen’s business strategy for its blockbuster Enbrel centered on matching price hikes by its biggest competitor, AbbVie’s Humira. Internal presentations reveal that Amgen planned its price hikes based on the behavior the company anticipated from AbbVie.
6. Pharma Claim: High prices fuel innovation.
The reality: Taxpayer funding fuels innovative new drugs. High prices fuel the growth of Big Pharma revenue. Drug companies don’t invest until public research shows commercial promise.
7. Pharma Claim: Pharmacy benefit managers are responsible for price increases.
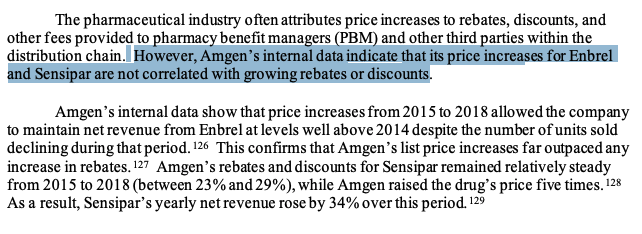
The reality: Big Pharma loves to point fingers, but internal documents show price increases on Amgen’s Enbrel and Sensipar are unrelated to rebates negotiated with PBMs. Instead, the price hikes are used to raise the company’s revenue.
Read our takeaways from yesterday’s reports from the House Oversight Committee into pharma giants Celgene and Teva.
###
By Sarah Kaminer Bourland, Legislative Director
1. Pharma Claim: High prices exist to recoup R&D, not drive profits.
The reality: Executives’ motivations for price hikes is devoid of desire to recoup or invest in R&D — instead the hikes are intended to increase revenue. Internal company documents showed that company executives weighed price increases against public backlash, not the actual impact on research and development funds. Ultimately, executives decided in favor of price hikes because “we will receive the same press regardless” and “any price increase obviously has positive results.”
2. Pharma Claim: We make life-saving drugs — it’s not about the money for us.
The reality: The committee’s investigation found that executive compensation policies incentivized price hikes. Novartis increased the price of Gleevec 22 times, and its revenue soared. As a result, more than 100 Novartis employees made $1 million in 2014 and 2015.
3. Pharma Claim: Our decision-making centers on the health and well-being of patients.
The reality:After public outrage at its $40,000 price for a single vial of Acthar Gel, Mallinckrodt’s CEO urged changing the vial size of Acthar gel (nearly cutting it in half) to appear like the company decreased the price.
4. Pharma Claim: Charity programs ensure our drugs are affordable and accessible.
The reality:Patient assistance programs serve both as a public relations tool for companies and to increase their bottom line. Novartis’ internal strategy documents estimated the rate of return of its co-pay assistance program would be $8.90 for every dollar invested. When weighing “key messages” to employ after a highly scrutinized price hike, one Novartis executive urged colleagues to emphasize contributions to the copay foundation.
5. Pharma Claim: It’s a robust marketplace and drug companies compete based on price.
The reality: Drug companies often collude — not compete. Amgen’s business strategy for its blockbuster Enbrel centered on matching price hikes by its biggest competitor, AbbVie’s Humira. Internal presentations reveal that Amgen planned its price hikes based on the behavior the company anticipated from AbbVie.
6. Pharma Claim: High prices fuel innovation.
The reality: Taxpayer funding fuels innovative new drugs. High prices fuel the growth of Big Pharma revenue. Drug companies don’t invest until public research shows commercial promise.
7. Pharma Claim: Pharmacy benefit managers are responsible for price increases.
The reality: Big Pharma loves to point fingers, but internal documents show price increases on Amgen’s Enbrel and Sensipar are unrelated to rebates negotiated with PBMs. Instead, the price hikes are used to raise the company’s revenue.
###
By Sarah Kaminer Bourland, Legislative Director
1. Pharma Claim: High prices exist to recoup R&D, not drive profits.
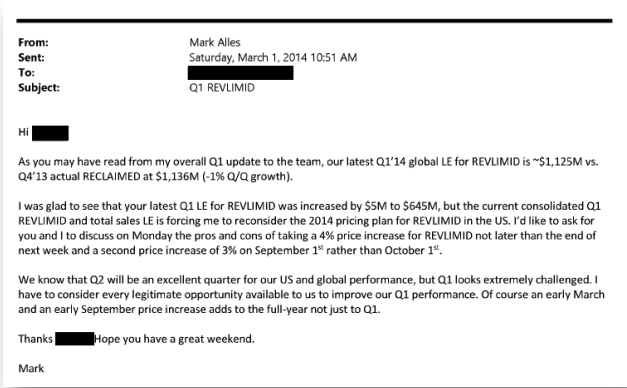
The reality: In a 2014 email from Mark Alles, Celgene’s CEO, the executive admits that he’s planning a price hike to meet sales targets. Furthermore, the investigation concluded that Celgene’s internal pricing decisions “were divorced from its calculus regarding future R&D or recouping of past R&D expenditures.”
2. Pharma Claim: We make life-saving drugs — it’s not about the money for us.
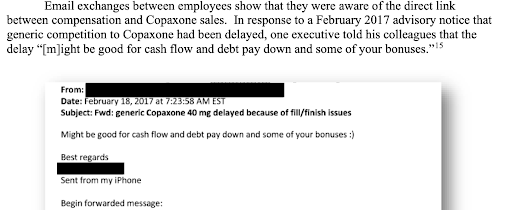
The reality: Instead of inviting a competitive market, drug companies thwart competitors at every turn. When news broke that a generic competitor had been delayed, Teva employees celebrated by exchanging emails about the financial implications for their bonuses.
3. Pharma Claim: Our decision-making centers on the safety and well-being of patients.
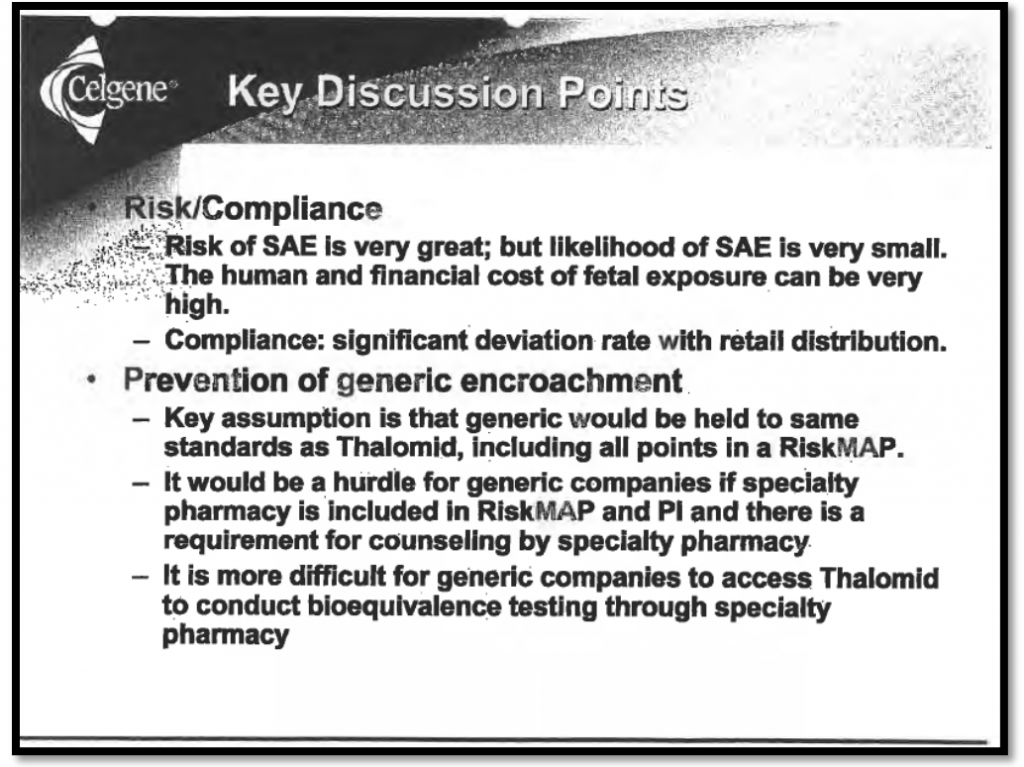
The reality:Celgene has long cited “safety” concerns as the company’s rationale for blocking generic competition through the FDA’s risk evaluation and mitigation strategies (REMS) program. But internal documents published today show that the company views their REMS program not as a means to promote safety, but as a tool to prevent “generic encroachment” and extend its monopoly.
4. Pharma Claim: Charity programs ensure our drugs are affordable and accessible.
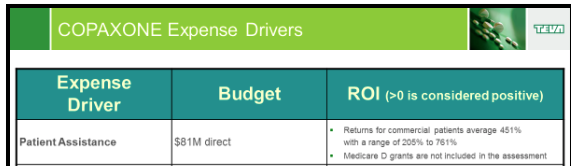
The reality:An internal presentation reveals that Teva averages a 451 percent return on every dollar invested in its copay assistance program. Teva’s program covers out-of-pocket expenses for patients while generating a full reimbursement for the drug corporation from each patient’s insurance company.
5. Pharma Claim: We support solutions to lower drug prices for patients.
The reality: Between 2017 and 2020, Teva spent $11.6 million lobbying Congress in order to thwart reforms that would harm its bottom line. According to internal documents, one of Celgene’s internal goals was to prevent the “legislative erosion” of the program it uses to prevent generics from coming to market.
6. Pharma Claim: High prices fuel new drugs.
The reality: Copaxone generated $34.2 billion in net U.S. revenue for Teva over nearly two decades. The drug corporation spent only 2 percent of that on R&D for the drug. Instead, Teva invested in developing “new” versions of old drugs that offer no therapeutic benefit.
7. Pharma Claim: Pharmacy benefit managers are responsible for price increases.
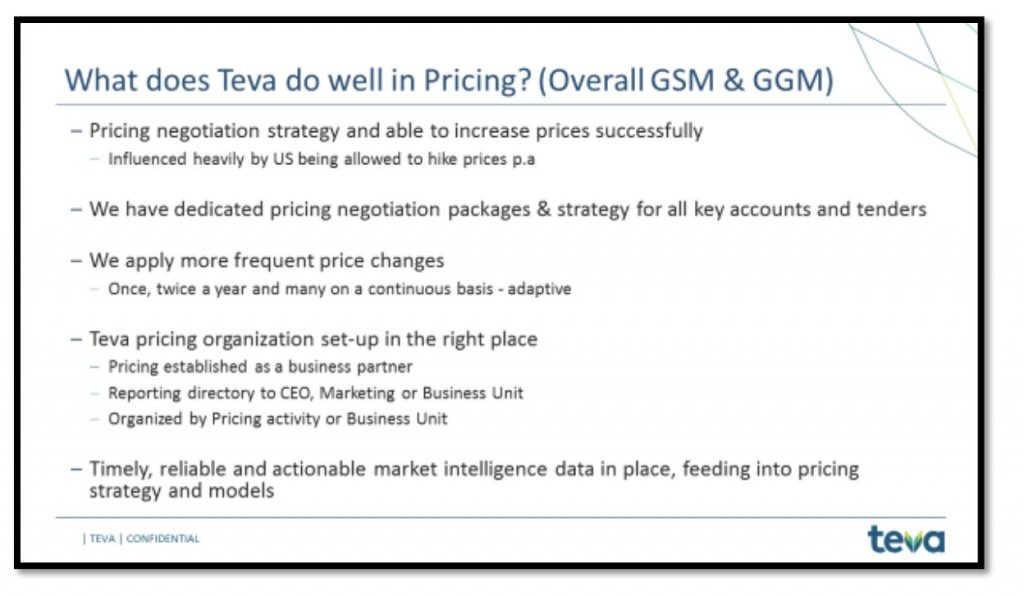
The reality: Drug companies alone set and control prices. In company PowerPoints, Teva boasted about its success increasing prices.
###
WASHINGTON, D.C. — Four patient advocates will deliver recorded testimonials before the House Committee on Oversight and Reform this week at hearings investigating drug company pricing practices. The patient advocates will share their experiences with four high-cost drugs made by pharmaceutical corporations under investigation by the committee.
“Millions of patients across America have been the victims of predatory pricing practices by drug corporations that prioritize profit maximization over public health,” said David Mitchell, a cancer patient and the founder of Patients For Affordable Drugs Now. “Today, patients will stand up to those companies and their CEOs, share their stories, and call on members of Congress to enact reforms to stop Big Pharma’s abusive practices.”
Read a copy of David Mitchell’s testimony submitted for the public record here.
Watch the patient advocates’ testimonials at the hearing here starting at 10 AM today. Below are some highlights of their stories:
Ramae Hamrin, Bemidji, MN, multiple myeloma: Ramae, a single mom with two kids in college, was diagnosed with multiple myeloma in 2018. She relies on Revlimid to stay healthy — but faces terrifying financial burdens to afford the very high price of her medication.
“In order to keep taking this drug, I will have to deplete my life savings, cash out my 401(k), and sell my house. When those funds run out, I’m not sure what I will do. Usually, I am a planner — but I cannot plan for this. I am terrified for my future.”
Therese Humphrey Ball, Portage, IN, multiple sclerosis: When Therese was first prescribed Copaxone in 2003, it cost $1,800 a month and wiped out her savings. By 2017, when Therese lost grant assistance, the price of the drug had risen to $6,000 a month, and Therese was forced to forgo the medication.
“When I was not on the drug, I lost short-term memory and experienced other declines in my cognitive functions. This makes it difficult for me to enjoy doing the things I love, like spending time with my grandchildren. My condition shouldn’t progress faster just because drug companies want to make a few extra bucks.”
Kip Burgess, Chicago, IL, psoriatic arthritis: Kip is a father, an avid cyclist, and a psychologist. At 30, he was diagnosed with psoriatic arthritis. In order to treat the debilitating pain that his condition causes, Kip takes Enbrel, a drug priced at $6,000 a month.
“If my ability to cover those costs goes away, I know I will go back to waking up every morning in pain. These risks cause crippling anxiety on top of the burden of the disease itself. In order to avoid these interruptions in my dosing, I’ve been forced to dip into my savings and jeopardize my financial health to preserve my physical health.”
Heidi Kendall, Missoula, MT, chronic myeloid leukemia: In 2017, Heidi was diagnosed with a blood cancer called chronic myeloid leukemia. To treat it, Heidi was prescribed the drug, Gleevec, which she must take every day for the rest of her life. The price tag is $10,000 per month.
“I’m so grateful for Gleevec. It keeps me alive. But the price tag constantly hangs over my head. Instead of just focusing on my family and my health, I also have to carry around the burden of what would happen if I couldn’t pay for it.”
The four drugs featured in the patient advocates’ testimonials are textbook examples of price gouging and patent abuse.
Revlimid, a cancer drug developed by Celgene and currently sold by Bristol Myers Squibb, costs Medicare more than almost any other drug but is used by fewer than 40,000 patients — less than 0.01 percent of beneficiaries. Celgene and BMS increased the price of the drug nearly 200 percent from 2007 to 2019 and have maintained monopoly pricing power far beyond the period intended by law.
Teva, the company that manufactures the multiple sclerosis medication Copaxone, is under scrutiny for engaging in anti-competitive practices such as product-hopping and shadow pricing that allow it to maintain its pricing power. Since 1997, the company has raised the price of Copaxone by more than 1,000 percent.
Enbrel is a blockbuster drug for Amgen, and the company has gone to extraordinary lengths to protect this revenue source, including leveraging 41 patents to delay generic competition.
Novartis quadrupled the price of its cancer drug, Gleevec, between 2001 and 2015. At the same time, the drug company entered into a collusive agreement with a generic manufacturer to delay less expensive competitors from entering the market.
The House Oversight and Reform committee’s probe into the drug industry was launched in January 2019 under then-chairman Rep. Elijah Cummings’ leadership. Over the past two years, the committee has investigated drug companies’ anti-competitive tactics by reviewing more than 1 million pages of internal documents. In addition to hearing from six current or former executives of top pharmaceutical companies over the next two days, the committee plans to subpoena pharma giant AbbVie for documents relating to its best-selling drugs Humira and Imbruvica.
The hearings begin today and will continue through tomorrow, starting at 10 AM ET each day. Watch the livestream here.
###
WASHINGTON, D.C. — During tonight’s debate at Case Western Reserve University, President Trump claimed that drug prices will be coming down by 80 to 90 percent.
FACT: President Trump hasn’t meaningfully lowered drug prices.
“Trump keeps claiming he lowered prescription drug prices. But that is largely not true” (Washington Post, 9/18/20)
“Trump misleads on lowering drug prices” (CNN Fact Check, 8/20/20)
“President Donald Trump exaggerated his administration’s efforts to lower prescription drug prices.” (Associated Press Fact Check, 9/9/20)
FACT: Drug prices keep rising.
“Drug prices steadily rise amid pandemic, data shows” (Politico, 7/7/20)
“Manufacturers hiked prices on 857 drugs by an average of 6.8% in the first six months of this year.” (CNN, 8/20/20)
“Since 2014, drug prices have increased by 33%, outpacing price increases for any other medical commodity or service.” (GoodRx, 9/17/20)
FACT: Patients are suffering under crushing drug prices and want change.
“Three in ten adults report not taking their medicines as prescribed at some point in the past year because of the cost.” (Kaiser Family Foundation, 3/1/19)
“Two-thirds of U.S. adults (66%) report that prescription drug prices have increased either a little or a lot since 2017, the first year of the Trump administration.” (Gallup, 4/28/20)
87% of Americans “say it is at least very important that Congress work on lowering prescription drug costs.” (Kaiser Family Foundation, 1/30/20)
FACT: President Trump’s executive orders, like the most-favored nation proposal, haven’t been put into practice.
“The president also claimed — inaccurately — that the ‘favored nations clause’ order had already lowered drug prices.” (New York Times, 8/24/20)
“It’s not true that Trump’s measures on favored nations and rebates are bringing prices down now — mainly because they haven’t gone into effect yet.” (CNN, 8/22/20)
“Most people are unlikely to see drug cost savings from President Trump’s ‘Most Favored Nation’ proposal.” (Kaiser Health News, 8/20/20)
“As with most executive actions, this only just begins what will be a lengthy bureaucratic process that may or may not ultimately result in the promised policy.” (NPR, 9/13/20)
“The nearly $7 billion required to send the coupons, he said, would come from savings from Trump’s ‘most favored nations’ drug pricing proposal. That regulation has also not yet been implemented — meaning the Trump administration is effectively pledging to spend $6.6 billion in savings that do not currently exist.” (STAT, 9/24/20)